{"title":"The impact of hemoadsorption in patients with chronic kidney disease undergoing coronary artery bypass grafting.","authors":"Erdal Simsek, Serdar Gunaydin","doi":"10.1093/ckj/sfaf241","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>With an annual incidence of up to 30%, cardiac surgery-associated acute kidney injury (CSA-AKI) may be one of the most underestimated yet common complications, hence reno-protective interventions are critical. We evaluated the impact of hemoadsorption (HA) on clinical outcomes in KDIGO (Kidney Disease: Improving Global Outcomes) G2/A2 patients (GFR 60-89 ml/min/1.73 m<sup>2</sup> and 30-300 mg/g albuminuria) undergoing coronary artery bypass grafting (CABG).</p><p><strong>Method: </strong>Forty patients with chronic kidney disease (KDIGO G2/A2) were treated with intraoperative HA therapy during CABG surgery (HA group) and were compared with 40 propensity-score matched control CABG patients without intraoperative HA (control group). Primary endpoints were the need for renal replacement therapy (RRT) and/or worsening of the KDIGO stage during the perioperative period. Secondary endpoints included changes in inflammatory biomarkers, vasopressor use, and ICU/hospital stay.</p><p><strong>Results: </strong>No significant differences were observed in demographics between groups. Worsened KDIGO stages were more frequent in the control group (<i>P</i> = .04), and the HA group had less RRT use and shorter ICU stays (<i>P</i> = .02 and <i>P</i> = .03). On the first postoperative day, levels of serum creatinine (1.85 ± 0.6 vs 2.75 ± 0.6 mg/dl; <i>P</i> = .035), myoglobin (210±75 vs 310 ± 80 μg/l; <i>P</i> = .04), NT-proBNP (130 ± 30 vs 180 ± 40 pg/ml; <i>P</i> = .04), IL-6 (8.2±4 vs 22.2 ± 4 pg/ml; <i>P</i> = .012), procalcitonin (1.4 ± 0.1 vs 1.76 ± 0.2 μg/l, <i>P</i> = .02), C-reactive protein (7.6 ± 2 vs 14.2 ± 4 mg/l, <i>P</i> = .01), and D-dimer (0.76 ± 0.04 vs 2.2 ± 0.07 mg/l, <i>P</i> = .002) were significantly lower in the HA group.</p><p><strong>Conclusion: </strong>This pioneering study highlights the potential benefits of HA in mitigating kidney function and inflammation in CABG patients with borderline chronic kidney disease. These findings require validation in large, multicenter trials.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 9","pages":"sfaf241"},"PeriodicalIF":4.6000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404029/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf241","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
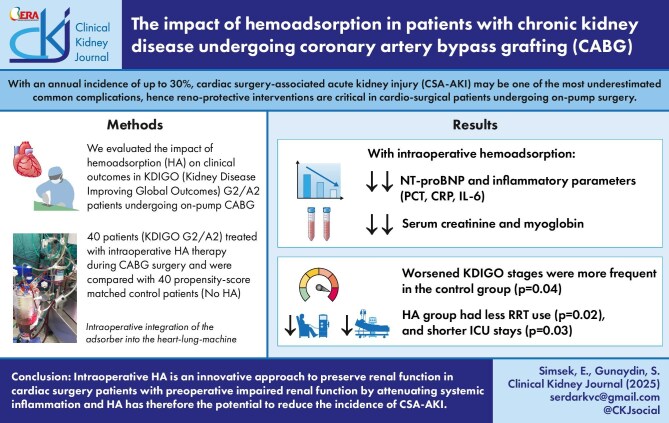
Background: With an annual incidence of up to 30%, cardiac surgery-associated acute kidney injury (CSA-AKI) may be one of the most underestimated yet common complications, hence reno-protective interventions are critical. We evaluated the impact of hemoadsorption (HA) on clinical outcomes in KDIGO (Kidney Disease: Improving Global Outcomes) G2/A2 patients (GFR 60-89 ml/min/1.73 m2 and 30-300 mg/g albuminuria) undergoing coronary artery bypass grafting (CABG).
Method: Forty patients with chronic kidney disease (KDIGO G2/A2) were treated with intraoperative HA therapy during CABG surgery (HA group) and were compared with 40 propensity-score matched control CABG patients without intraoperative HA (control group). Primary endpoints were the need for renal replacement therapy (RRT) and/or worsening of the KDIGO stage during the perioperative period. Secondary endpoints included changes in inflammatory biomarkers, vasopressor use, and ICU/hospital stay.
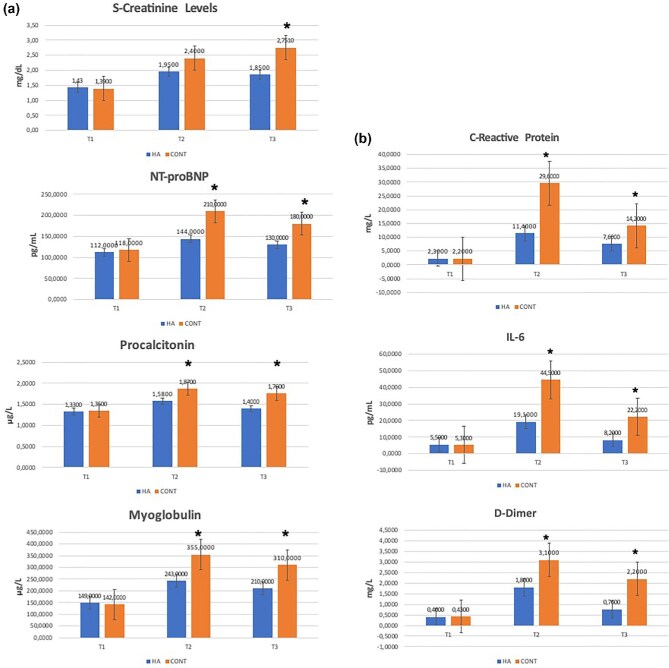
Results: No significant differences were observed in demographics between groups. Worsened KDIGO stages were more frequent in the control group (P = .04), and the HA group had less RRT use and shorter ICU stays (P = .02 and P = .03). On the first postoperative day, levels of serum creatinine (1.85 ± 0.6 vs 2.75 ± 0.6 mg/dl; P = .035), myoglobin (210±75 vs 310 ± 80 μg/l; P = .04), NT-proBNP (130 ± 30 vs 180 ± 40 pg/ml; P = .04), IL-6 (8.2±4 vs 22.2 ± 4 pg/ml; P = .012), procalcitonin (1.4 ± 0.1 vs 1.76 ± 0.2 μg/l, P = .02), C-reactive protein (7.6 ± 2 vs 14.2 ± 4 mg/l, P = .01), and D-dimer (0.76 ± 0.04 vs 2.2 ± 0.07 mg/l, P = .002) were significantly lower in the HA group.
Conclusion: This pioneering study highlights the potential benefits of HA in mitigating kidney function and inflammation in CABG patients with borderline chronic kidney disease. These findings require validation in large, multicenter trials.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


