Jorge E Rojas-Rivera, Fernando Caravaca-Fontán, Anne-Els van de Logt, Angel Sevillano, Amir Shabaka, Ana Ávila, Cristina Rabasco, Virginia Cabello, Alberto Ortiz, Luis F Quintana, Marian Goicoechea, Montserrat Diaz, Pierre Ronco, Jack Wetzels, Gema Fernández-Juárez, Manuel Praga
{"title":"Identification of early predictors of clinical remission in primary membranous nephropathy: a <i>post hoc</i> analysis of the STARMEN trial.","authors":"Jorge E Rojas-Rivera, Fernando Caravaca-Fontán, Anne-Els van de Logt, Angel Sevillano, Amir Shabaka, Ana Ávila, Cristina Rabasco, Virginia Cabello, Alberto Ortiz, Luis F Quintana, Marian Goicoechea, Montserrat Diaz, Pierre Ronco, Jack Wetzels, Gema Fernández-Juárez, Manuel Praga","doi":"10.1093/ckj/sfaf256","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with primary membranous nephropathy may progress to advanced chronic kidney disease despite immunosuppressive therapy (IST). Prediction of treatment response based on early and combined assessment of several standard clinical markers could improve risk stratification for progression, allowing timely individualization of treatment, which can optimize clinical outcomes and safety.</p><p><strong>Methods: </strong>In this <i>post hoc</i> exploratory analysis of the STARMEN trial, we evaluated if combined baseline data, and IST-induced early changes in standard clinical markers predicted clinical remission at 2 years. The 2-year primary outcome was complete (CR) or partial remission (PR). The secondary outcome was CR. Additionally, we described kidney function outcomes. Standard clinical markers were incorporated into statistical modeling by logistic regression. Predictive performance was assessed by receiver operating characteristic curve analysis.</p><p><strong>Results: </strong>The best multivariate model excluding immunosuppression to predict complete or PR at 2 years, included 3-month 24-h proteinuria, serum creatinine and immunological response [area under the curve (AUC) 0.87, 95% confidence interval (CI) 0.76-0.94, efficiency 87%]. For CR at 2 years, the best model included the same clinical markers at 6 months, but predictive performance was lower (AUC 0.74, 95% CI 0.62-0.85, efficiency 70%).</p><p><strong>Conclusions: </strong>In the STARMEN cohort, a multivariable model that included 24-h proteinuria, serum creatinine and immunological response status at 3 months after initiation of IST predicted clinical remission at 2 years with significantly better predictive performance than baseline data or each clinical marker assessed separately.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 9","pages":"sfaf256"},"PeriodicalIF":4.6000,"publicationDate":"2025-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399971/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf256","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with primary membranous nephropathy may progress to advanced chronic kidney disease despite immunosuppressive therapy (IST). Prediction of treatment response based on early and combined assessment of several standard clinical markers could improve risk stratification for progression, allowing timely individualization of treatment, which can optimize clinical outcomes and safety.
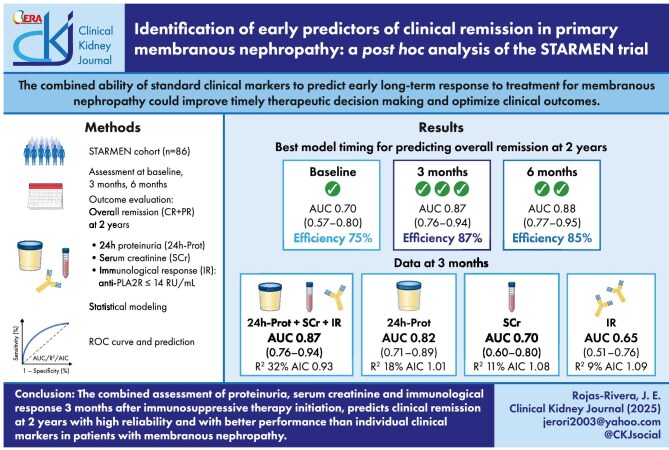
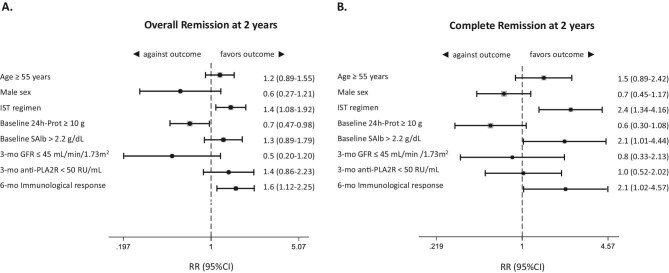
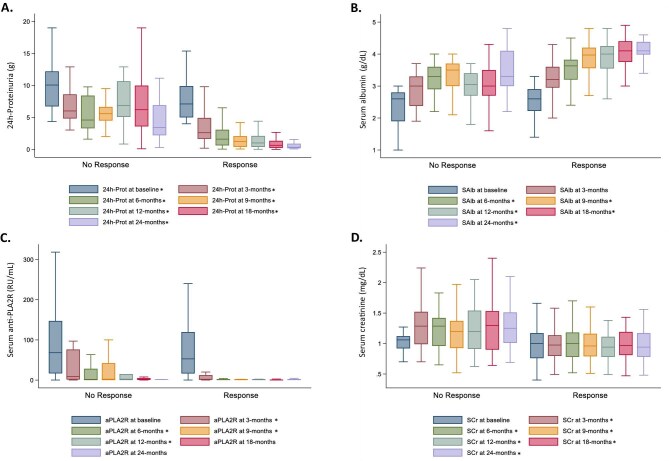
Methods: In this post hoc exploratory analysis of the STARMEN trial, we evaluated if combined baseline data, and IST-induced early changes in standard clinical markers predicted clinical remission at 2 years. The 2-year primary outcome was complete (CR) or partial remission (PR). The secondary outcome was CR. Additionally, we described kidney function outcomes. Standard clinical markers were incorporated into statistical modeling by logistic regression. Predictive performance was assessed by receiver operating characteristic curve analysis.
Results: The best multivariate model excluding immunosuppression to predict complete or PR at 2 years, included 3-month 24-h proteinuria, serum creatinine and immunological response [area under the curve (AUC) 0.87, 95% confidence interval (CI) 0.76-0.94, efficiency 87%]. For CR at 2 years, the best model included the same clinical markers at 6 months, but predictive performance was lower (AUC 0.74, 95% CI 0.62-0.85, efficiency 70%).
Conclusions: In the STARMEN cohort, a multivariable model that included 24-h proteinuria, serum creatinine and immunological response status at 3 months after initiation of IST predicted clinical remission at 2 years with significantly better predictive performance than baseline data or each clinical marker assessed separately.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


