Sai Nikhitha Malapati, Ashok Adhikari, Venkata Akhil Makarla, Sai Geethika Malapati, Krishnam Raju Dema, Apsha Shrestha
{"title":"Endoscopic thulium-fiber laser deroofing and dual stenting for adult duplex ureterocele with preserved upper renal moiety: a case report.","authors":"Sai Nikhitha Malapati, Ashok Adhikari, Venkata Akhil Makarla, Sai Geethika Malapati, Krishnam Raju Dema, Apsha Shrestha","doi":"10.1097/MS9.0000000000003704","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adult duplex kidney with ureterocele is rarely diagnosed, especially when the upper moiety retains function. While pediatric laser decompression is established, the use of thulium fiber laser (TFL) with dual DJ stenting in adult duplex ureteroceles remains rare.</p><p><strong>Case presentation: </strong>A 23-year-old female presented in a tertiary care hospital with intermittent right flank pain and recurrent UTIs for 3 months. Imaging revealed a right-sided duplex system with an intravesical ureterocele and functioning upper moiety. TFL deroofing was performed, with placement of dual DJ stents. Operative time was 40 minutes with negligible bleeding. Recovery was uneventful, and stents were removed at 6 weeks. At 6 months, imaging confirmed resolved hydronephrosis and preserved function; the patient remained asymptomatic at 12-month tele-follow-up.</p><p><strong>Clinical discussion: </strong>Ureteroceles result from ureteric bud maldevelopment and are often associated with duplex systems per the Weigert-Meyer law. Adult presentations may include recurrent UTIs, hematuria, or flank pain. Imaging modalities such as ultrasonography, CT urography, and renography are essential for diagnosis and surgical planning that prioritizes decompression and nephron preservation. Traditional endoscopic methods, including cold-knife incision and Holmium:YAG laser, risk reflux and tissue damage. TFL offers precise, shallow ablation with better hemostasis and reduced complications, though its adult use is underreported. This case represents the first documented TFL deroofing with dual DJ stenting in adult duplex ureterocele, showing excellent anatomical and functional outcomes, suggesting TFL's potential as a safe, effective option pending larger studies.</p><p><strong>Conclusion: </strong>TFL with dual DJ stenting offers a precise, nephron-preserving, and effective approach for adult ureterocele management.</p>","PeriodicalId":8025,"journal":{"name":"Annals of Medicine and Surgery","volume":"87 9","pages":"6221-6225"},"PeriodicalIF":1.6000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401281/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Medicine and Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/MS9.0000000000003704","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adult duplex kidney with ureterocele is rarely diagnosed, especially when the upper moiety retains function. While pediatric laser decompression is established, the use of thulium fiber laser (TFL) with dual DJ stenting in adult duplex ureteroceles remains rare.
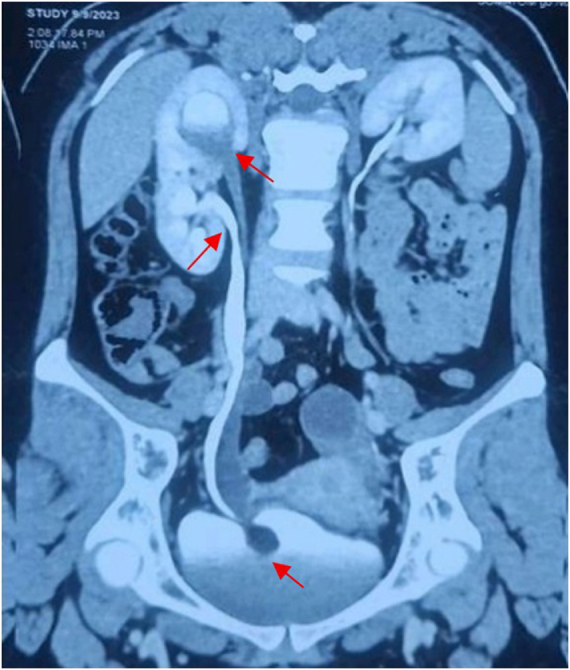
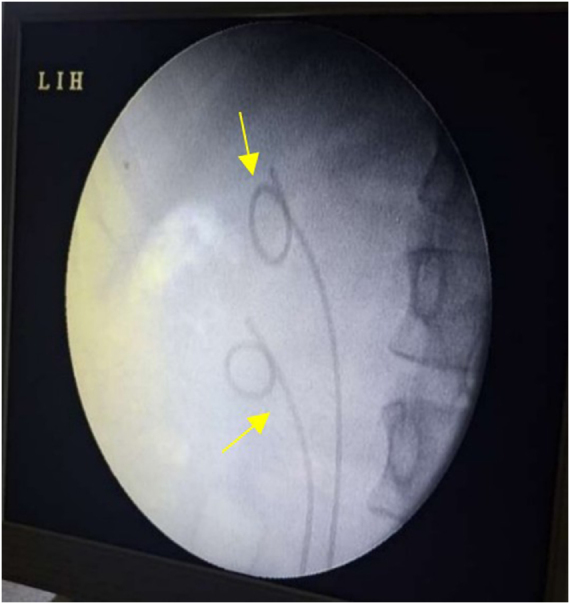
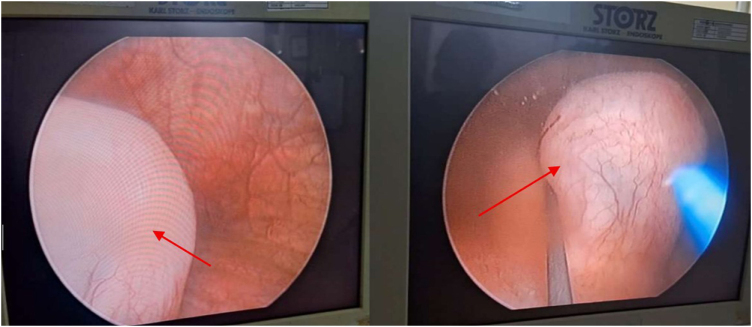
Case presentation: A 23-year-old female presented in a tertiary care hospital with intermittent right flank pain and recurrent UTIs for 3 months. Imaging revealed a right-sided duplex system with an intravesical ureterocele and functioning upper moiety. TFL deroofing was performed, with placement of dual DJ stents. Operative time was 40 minutes with negligible bleeding. Recovery was uneventful, and stents were removed at 6 weeks. At 6 months, imaging confirmed resolved hydronephrosis and preserved function; the patient remained asymptomatic at 12-month tele-follow-up.
Clinical discussion: Ureteroceles result from ureteric bud maldevelopment and are often associated with duplex systems per the Weigert-Meyer law. Adult presentations may include recurrent UTIs, hematuria, or flank pain. Imaging modalities such as ultrasonography, CT urography, and renography are essential for diagnosis and surgical planning that prioritizes decompression and nephron preservation. Traditional endoscopic methods, including cold-knife incision and Holmium:YAG laser, risk reflux and tissue damage. TFL offers precise, shallow ablation with better hemostasis and reduced complications, though its adult use is underreported. This case represents the first documented TFL deroofing with dual DJ stenting in adult duplex ureterocele, showing excellent anatomical and functional outcomes, suggesting TFL's potential as a safe, effective option pending larger studies.
Conclusion: TFL with dual DJ stenting offers a precise, nephron-preserving, and effective approach for adult ureterocele management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


