The prognostic values of monitoring changes in coagulative, inflammatory, and blood chemistry markers in COVID-19 patient's before and during admission to ICU: a retrospective cohort study.
Amer Hashim Al Ani, Gabriel Andrade, Yara Elsherbiny, Afiya Walid Zaynob, Mesk Alhammadi, Kowthar Forsat, Vidya Jakapure
{"title":"The prognostic values of monitoring changes in coagulative, inflammatory, and blood chemistry markers in COVID-19 patient's before and during admission to ICU: a retrospective cohort study.","authors":"Amer Hashim Al Ani, Gabriel Andrade, Yara Elsherbiny, Afiya Walid Zaynob, Mesk Alhammadi, Kowthar Forsat, Vidya Jakapure","doi":"10.1097/MS9.0000000000003600","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The infection caused by the COVID-19 virus is associated with thromboembolic events and severe inflammatory reactions, significantly impacting the prognosis of infected patients. Numerous studies have indicated that COVID-19 patients often exhibit a hypercoagulable state, disseminated intravascular coagulation, and overwhelming inflammation, particularly in critically ill patients with multiple comorbidities requiring admission to the ICU. This study aims to assess the prognostic significance of alterations in coagulation, inflammatory, and blood chemistry markers in COVID-19 patients both before and during admission to the ICU.</p><p><strong>Methods: </strong>Study design and population: This retrospective observational cohort study was conducted from March 2020 to July 2021 at a single center, including 90 adult patients with confirmed COVID-19 infection requiring ICU admission. Patients were divided into two groups: survivors (<i>n</i> = 42) and non-survivors (<i>n</i> = 48). The median age of non-survivors was 48.5 years (BMI 26-40), while survivors had a median age of 54 years (BMI 23-35). All participants received uniform supportive therapy comprising endotracheal intubation, anticoagulation (low molecular weight heparin or unfractionated heparin), aspirin, and steroids. No antiviral therapy was administered. Inclusion criteria encompassed adult COVID-19-positive patients requiring ICU admission. Exclusion criteria included pediatric patients, adult COVID-19 patients not admitted to the ICU, and Intensive Care Unit (ICU) patients without COVID-19 infection. Data collection: Demographic data (age, gender, comorbidities) and laboratory parameters (D-dimer, lactate dehydrogenase [LDH], procalcitonin, prothrombin time, platelet count, ferritin, C-reactive protein [CRP], glucose, and creatinine) were extracted from electronic medical records at three time points: ICU admission, shortly after treatment initiation, and at discharge or death. Statistical analysis: A total of 94 patients were initially assessed; three were excluded due to incomplete data, yielding a final cohort of 91 patients. Missing data for certain variables were imputed using the median of respective variables. Given the non-normal distribution of most laboratory markers, non-parametric statistical tests were applied. Paired Wilcoxon signed-rank tests were used to compare biomarker medians between admission and subsequent time points. Mann-Whitney <i>U</i> tests were employed to evaluate differences between survivors and non-survivors. All tests were two-tailed with a significance threshold set at <i>P</i> ≤ 0.05. Analyses were performed using Jamovi software.</p><p><strong>Results: </strong>Baseline characteristics: A total of 91 patients were included in the final analysis, comprising 42 survivors (36 males [83.7%], 6 females [16.3%]; median age 54 years [Interquartile Range (IQR): 49-59]; Body Mass Index (BMI) range 23-35) and 48 non-survivors (40 males [83.3%], 8 females [16.7%]; median age 48.5 years [IQR: 45-53]; BMI range 26-40). Overall, the cohort was predominantly male (83.5%) and had a wide range of body mass index. At ICU admission, survivors had slightly higher median platelet counts (257 vs 254 × 10<sup>9</sup>/L) and ferritin levels (1491 vs 1212 ng/mL), whereas non-survivors had higher median D-dimer (3.33 vs 2.28 mg/L), CRP (185 vs 131 mg/L), and procalcitonin (0.825 vs 0.51 ng/mL) levels. Creatinine, LDH, and glucose levels were similar between the groups at admission. Baseline demographic and clinical characteristics, along with initial laboratory values, are summarized in Table 1. Temporal changes in biomarker levels: Serial measurements revealed significant biomarker changes across the ICU stay. In the overall cohort, the Wilcoxon signed-rank test identified significant increases in platelet count (median 256 to 294 × 10<sup>9</sup>/L, <i>P</i> < 0.001) and procalcitonin levels (median 0.6-0.93 ng/mL, <i>P</i> = 0.016) shortly after treatment initiation (Table 2). From admission to discharge or death, significant increases were observed in prothrombin time (median 14.5-15.2 s, p<0.001), procalcitonin (median 0.6-1.01 ng/mL, <i>P</i> < 0.001), and creatinine (median 78-92 µmol/L, <i>P</i> < 0.001), whereas CRP (median 172.5-61.2 mg/L, <i>P</i> < 0.001) and LDH (median 581-472 U/L, <i>P</i> = 0.001) significantly decreased (Table 3). These temporal dynamics are visually summarized in Figure 1 (panels A-E), displaying median and mean values with 95% confidence intervals for each biomarker. Comparisons between survivors and non-survivors: Mann-Whitney <i>U</i> test comparisons (Table 4) revealed significant differences between survivors and non-survivors. At admission, survivors had significantly lower glucose levels (median 10.8 vs 8.2 mmol/L, <i>P</i> = 0.006). Shortly after treatment, survivors exhibited lower D-dimer (<i>P</i> = 0.013), prothrombin time (<i>P</i> = 0.022), ferritin (<i>P</i> = 0.022), CRP (<i>P</i> = 0.028), and LDH (<i>P</i> = 0.003) levels compared to non-survivors. At discharge or death, survivors demonstrated significantly higher platelet counts (median 331 vs 211 × 10<sup>9</sup>/L, <i>P</i> < 0.001) and significantly lower D-dimer, prothrombin time, ferritin, CRP, procalcitonin, creatinine, and LDH levels (all <i>P</i> < 0.001). Subgroup analyses: Among non-survivors, significant increases in prothrombin time, ferritin, procalcitonin, and creatinine levels were observed between admission and shortly before death, alongside a decrease in platelet count (all <i>P</i> < 0.001). Conversely, survivors showed significant reductions in CRP, ferritin, procalcitonin, and glucose at discharge (all <i>P</i> < 0.001), accompanied by increased platelet counts (median 257-331 × 10<sup>9</sup>/L, <i>P</i> < 0.001) and decreased LDH (median 570-472 U/L, <i>P</i> = 0.001).</p><p><strong>Conclusion: </strong>This study identifies key biomarkers that predict COVID-19 outcomes, emphasizing the association between platelet count and the final fate of COVID-19 patients admitted to the ICU. Elevated ferritin levels predict disease deterioration and poor prognosis, whereas lower glucose levels indicate a better prognosis.</p>","PeriodicalId":8025,"journal":{"name":"Annals of Medicine and Surgery","volume":"87 9","pages":"5401-5408"},"PeriodicalIF":1.6000,"publicationDate":"2025-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401196/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Medicine and Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/MS9.0000000000003600","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The infection caused by the COVID-19 virus is associated with thromboembolic events and severe inflammatory reactions, significantly impacting the prognosis of infected patients. Numerous studies have indicated that COVID-19 patients often exhibit a hypercoagulable state, disseminated intravascular coagulation, and overwhelming inflammation, particularly in critically ill patients with multiple comorbidities requiring admission to the ICU. This study aims to assess the prognostic significance of alterations in coagulation, inflammatory, and blood chemistry markers in COVID-19 patients both before and during admission to the ICU.
Methods: Study design and population: This retrospective observational cohort study was conducted from March 2020 to July 2021 at a single center, including 90 adult patients with confirmed COVID-19 infection requiring ICU admission. Patients were divided into two groups: survivors (n = 42) and non-survivors (n = 48). The median age of non-survivors was 48.5 years (BMI 26-40), while survivors had a median age of 54 years (BMI 23-35). All participants received uniform supportive therapy comprising endotracheal intubation, anticoagulation (low molecular weight heparin or unfractionated heparin), aspirin, and steroids. No antiviral therapy was administered. Inclusion criteria encompassed adult COVID-19-positive patients requiring ICU admission. Exclusion criteria included pediatric patients, adult COVID-19 patients not admitted to the ICU, and Intensive Care Unit (ICU) patients without COVID-19 infection. Data collection: Demographic data (age, gender, comorbidities) and laboratory parameters (D-dimer, lactate dehydrogenase [LDH], procalcitonin, prothrombin time, platelet count, ferritin, C-reactive protein [CRP], glucose, and creatinine) were extracted from electronic medical records at three time points: ICU admission, shortly after treatment initiation, and at discharge or death. Statistical analysis: A total of 94 patients were initially assessed; three were excluded due to incomplete data, yielding a final cohort of 91 patients. Missing data for certain variables were imputed using the median of respective variables. Given the non-normal distribution of most laboratory markers, non-parametric statistical tests were applied. Paired Wilcoxon signed-rank tests were used to compare biomarker medians between admission and subsequent time points. Mann-Whitney U tests were employed to evaluate differences between survivors and non-survivors. All tests were two-tailed with a significance threshold set at P ≤ 0.05. Analyses were performed using Jamovi software.
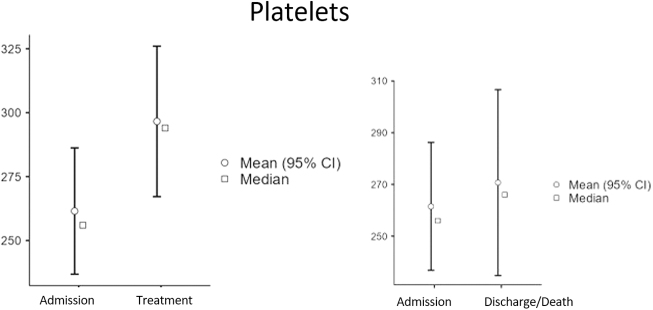
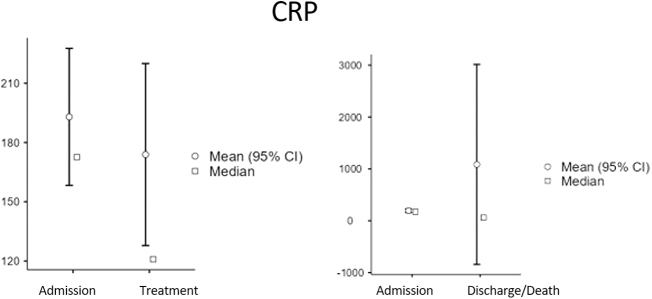
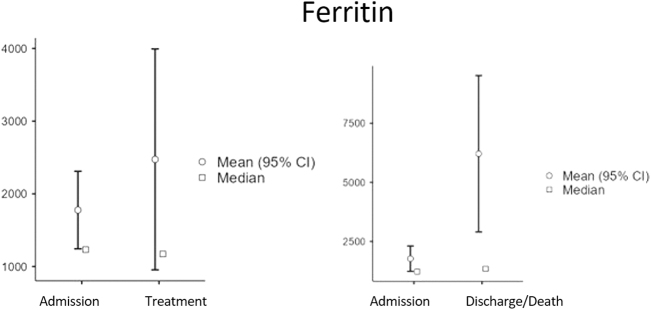
Results: Baseline characteristics: A total of 91 patients were included in the final analysis, comprising 42 survivors (36 males [83.7%], 6 females [16.3%]; median age 54 years [Interquartile Range (IQR): 49-59]; Body Mass Index (BMI) range 23-35) and 48 non-survivors (40 males [83.3%], 8 females [16.7%]; median age 48.5 years [IQR: 45-53]; BMI range 26-40). Overall, the cohort was predominantly male (83.5%) and had a wide range of body mass index. At ICU admission, survivors had slightly higher median platelet counts (257 vs 254 × 109/L) and ferritin levels (1491 vs 1212 ng/mL), whereas non-survivors had higher median D-dimer (3.33 vs 2.28 mg/L), CRP (185 vs 131 mg/L), and procalcitonin (0.825 vs 0.51 ng/mL) levels. Creatinine, LDH, and glucose levels were similar between the groups at admission. Baseline demographic and clinical characteristics, along with initial laboratory values, are summarized in Table 1. Temporal changes in biomarker levels: Serial measurements revealed significant biomarker changes across the ICU stay. In the overall cohort, the Wilcoxon signed-rank test identified significant increases in platelet count (median 256 to 294 × 109/L, P < 0.001) and procalcitonin levels (median 0.6-0.93 ng/mL, P = 0.016) shortly after treatment initiation (Table 2). From admission to discharge or death, significant increases were observed in prothrombin time (median 14.5-15.2 s, p<0.001), procalcitonin (median 0.6-1.01 ng/mL, P < 0.001), and creatinine (median 78-92 µmol/L, P < 0.001), whereas CRP (median 172.5-61.2 mg/L, P < 0.001) and LDH (median 581-472 U/L, P = 0.001) significantly decreased (Table 3). These temporal dynamics are visually summarized in Figure 1 (panels A-E), displaying median and mean values with 95% confidence intervals for each biomarker. Comparisons between survivors and non-survivors: Mann-Whitney U test comparisons (Table 4) revealed significant differences between survivors and non-survivors. At admission, survivors had significantly lower glucose levels (median 10.8 vs 8.2 mmol/L, P = 0.006). Shortly after treatment, survivors exhibited lower D-dimer (P = 0.013), prothrombin time (P = 0.022), ferritin (P = 0.022), CRP (P = 0.028), and LDH (P = 0.003) levels compared to non-survivors. At discharge or death, survivors demonstrated significantly higher platelet counts (median 331 vs 211 × 109/L, P < 0.001) and significantly lower D-dimer, prothrombin time, ferritin, CRP, procalcitonin, creatinine, and LDH levels (all P < 0.001). Subgroup analyses: Among non-survivors, significant increases in prothrombin time, ferritin, procalcitonin, and creatinine levels were observed between admission and shortly before death, alongside a decrease in platelet count (all P < 0.001). Conversely, survivors showed significant reductions in CRP, ferritin, procalcitonin, and glucose at discharge (all P < 0.001), accompanied by increased platelet counts (median 257-331 × 109/L, P < 0.001) and decreased LDH (median 570-472 U/L, P = 0.001).
Conclusion: This study identifies key biomarkers that predict COVID-19 outcomes, emphasizing the association between platelet count and the final fate of COVID-19 patients admitted to the ICU. Elevated ferritin levels predict disease deterioration and poor prognosis, whereas lower glucose levels indicate a better prognosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


