{"title":"The first case report of chylous ascites in a twin pregnancy following <i>in vitro</i> fertilization: a case report of chylous ascites in twin pregnancy.","authors":"Nguyen Xuan Hoi, Nguyen Thi Huyen Anh, Phung Thi Ly, Nguyen Dang Tuan","doi":"10.1097/MS9.0000000000003686","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction and importance: </strong>Chylous ascites is an exceptionally rare condition during pregnancy, typically presenting with nonspecific symptoms. To date, only a limited number of cases have been reported in the literature, and the majority of which occurred in singleton pregnancies.</p><p><strong>Case presentation: </strong>We report the case of a 25-year-old woman with a twin pregnancy who was admitted at 32 weeks of gestation with acute abdominal pain and nausea. Due to persistent severe pain, unexplained intraperitoneal fluid, and progressing labor, an emergent cesarean section was performed. Intraoperatively, 2000 mL of milky white fluid was discovered in the peritoneal cavity. Biochemical analysis with markedly elevated triglycerides confirmed the diagnosis of chylous ascites. Postoperative management included broad-spectrum intravenous antibiotics, octreotide injection, and a low-fat diet supplemented with medium-chain triglyceride oil. By postoperative day 7, ultrasound showed complete resolution of ascites, and the patient was discharged in stable condition. No recurrence was noted during 3 years of follow-up.</p><p><strong>Clinical discussion: </strong>This report presents a rare case of spontaneous chylous ascites in a previously healthy pregnant woman with a twin gestation. Potential mechanism for chylous ascites in our case can be due to enlarged gravid uterus of twin gestation during late pregnancy, which suppress the abdominal thoracic duct of mother and increase the pressure of the duct. Another possible mechanism involves the physiological effects of progesterone during pregnancy. Progesterone is known to induce smooth muscle relaxation, which can lead to dilation of lymphatic vessels and increased lymphatic flow. This vasodilatory effect may predispose to lymphatic leakage and contribute to the development of chylous ascites. The presence of milky white peritoneal fluid combined with a markedly elevated triglyceride concentration (≥ 110 mg/dL, 1945 mg/dL in our case) was key to confirm the diagnosis of chylous ascites. Treatment strategies typically depends on the underlying etiology and may include dietary modification (low-fat, MCT-enriched diet), pharmacologic therapy (somatostatin or octreotide), and surgical interventions in refractory cases.</p><p><strong>Conclusion: </strong>Chylous ascites should be included in the differential diagnosis of unexplained ascites in twin gestation, particularly when the fluid exhibits a milky appearance. Although chylous ascites resolves spontaneously in the postpartum period, this condition may necessitate the termination of pregnancy and requires a multidisciplinary approach, involving obstetricians, gastrointestinal surgeons, radiologists, and nutritionists, for timely diagnosis and effective management.</p>","PeriodicalId":8025,"journal":{"name":"Annals of Medicine and Surgery","volume":"87 9","pages":"6211-6215"},"PeriodicalIF":1.6000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401213/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Medicine and Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/MS9.0000000000003686","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction and importance: Chylous ascites is an exceptionally rare condition during pregnancy, typically presenting with nonspecific symptoms. To date, only a limited number of cases have been reported in the literature, and the majority of which occurred in singleton pregnancies.
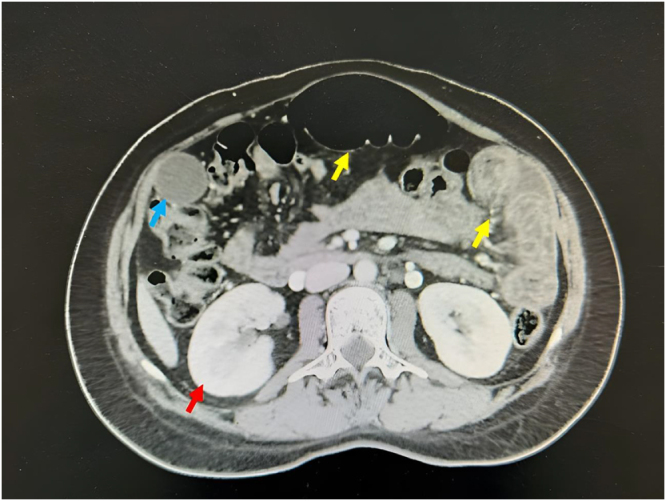
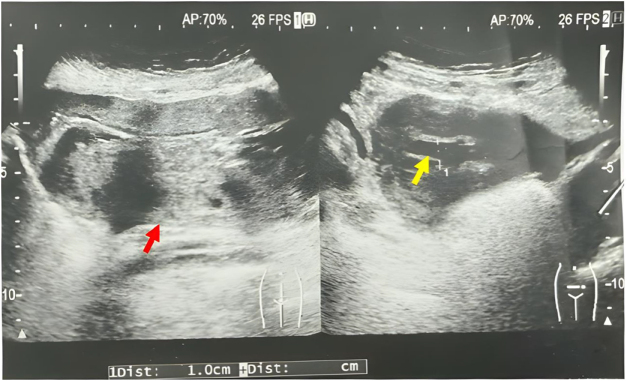
Case presentation: We report the case of a 25-year-old woman with a twin pregnancy who was admitted at 32 weeks of gestation with acute abdominal pain and nausea. Due to persistent severe pain, unexplained intraperitoneal fluid, and progressing labor, an emergent cesarean section was performed. Intraoperatively, 2000 mL of milky white fluid was discovered in the peritoneal cavity. Biochemical analysis with markedly elevated triglycerides confirmed the diagnosis of chylous ascites. Postoperative management included broad-spectrum intravenous antibiotics, octreotide injection, and a low-fat diet supplemented with medium-chain triglyceride oil. By postoperative day 7, ultrasound showed complete resolution of ascites, and the patient was discharged in stable condition. No recurrence was noted during 3 years of follow-up.
Clinical discussion: This report presents a rare case of spontaneous chylous ascites in a previously healthy pregnant woman with a twin gestation. Potential mechanism for chylous ascites in our case can be due to enlarged gravid uterus of twin gestation during late pregnancy, which suppress the abdominal thoracic duct of mother and increase the pressure of the duct. Another possible mechanism involves the physiological effects of progesterone during pregnancy. Progesterone is known to induce smooth muscle relaxation, which can lead to dilation of lymphatic vessels and increased lymphatic flow. This vasodilatory effect may predispose to lymphatic leakage and contribute to the development of chylous ascites. The presence of milky white peritoneal fluid combined with a markedly elevated triglyceride concentration (≥ 110 mg/dL, 1945 mg/dL in our case) was key to confirm the diagnosis of chylous ascites. Treatment strategies typically depends on the underlying etiology and may include dietary modification (low-fat, MCT-enriched diet), pharmacologic therapy (somatostatin or octreotide), and surgical interventions in refractory cases.
Conclusion: Chylous ascites should be included in the differential diagnosis of unexplained ascites in twin gestation, particularly when the fluid exhibits a milky appearance. Although chylous ascites resolves spontaneously in the postpartum period, this condition may necessitate the termination of pregnancy and requires a multidisciplinary approach, involving obstetricians, gastrointestinal surgeons, radiologists, and nutritionists, for timely diagnosis and effective management.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


