Aliya N Bryce, Brett Sobey, Paul Kinsella, Steven Y C Tong, Nigel D Toussaint
{"title":"Clinical Characteristics, Microbiology and Outcomes of Bloodstream Infections in Patients Undergoing Haemodialysis-An Australian Network Cohort Study.","authors":"Aliya N Bryce, Brett Sobey, Paul Kinsella, Steven Y C Tong, Nigel D Toussaint","doi":"10.1111/nep.70113","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>This study reviewed the morbidity and mortality of bloodstream infections (BSIs) in patients with kidney failure receiving haemodialysis (HD).</p><p><strong>Methods: </strong>We conducted a retrospective cohort study reviewing clinical characteristics, microbiology and outcomes of BSIs in patients receiving HD from 1 December 2017 to 1 December 2023 using data from an integrated network of dialysis sites. Descriptive and regression analyses were conducted, as well as Kaplan-Meier analysis for survival.</p><p><strong>Results: </strong>Of 1461 patients who received HD over the study period, 171 positive blood cultures occurred in 137 patients. Sixty blood cultures (35%) were considered non-significant contaminants, leaving 111 significant BSIs in 97 patients. Patients with BSIs had a median age of 65 years (interquartile range [IQR]: 50-76); 61% were males, with 48% having diabetes mellitus and 57% cardiovascular disease. A high proportion of BSI episodes (66/111, 59%) were determined to be HD access-associated, primarily in patients with central venous catheters (55/111, 50%). The most frequent non-HD access-associated sources were intra-abdominal/biliary (9%) and urinary (8%). Staphylococcus aureus (25%) was the most isolated organism, followed by Staphylococcus epidermis (12%). Polymicrobial BSI occurred in 10% of episodes. Median hospitalisation length was 9 days (IQR: 6-15). Mortality at 90 days was high (24%), and on multivariate analysis was associated with increasing age (odds ratio: 1.06 per year [IQR: 1.01-1.10]).</p><p><strong>Conclusion: </strong>BSIs remain a major issue in patients receiving HD, contributing to prolonged hospitalisations and high mortality rates. HD access-associated BSIs account for a substantial proportion of BSIs and remain a pertinent target for intervention.</p>","PeriodicalId":520716,"journal":{"name":"Nephrology (Carlton, Vic.)","volume":"30 9","pages":"e70113"},"PeriodicalIF":1.9000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377933/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephrology (Carlton, Vic.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1111/nep.70113","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: This study reviewed the morbidity and mortality of bloodstream infections (BSIs) in patients with kidney failure receiving haemodialysis (HD).
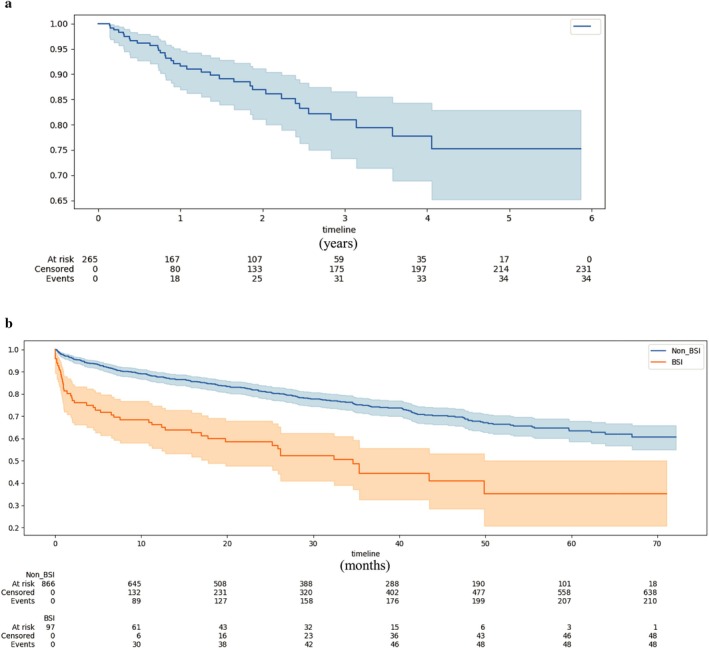
Methods: We conducted a retrospective cohort study reviewing clinical characteristics, microbiology and outcomes of BSIs in patients receiving HD from 1 December 2017 to 1 December 2023 using data from an integrated network of dialysis sites. Descriptive and regression analyses were conducted, as well as Kaplan-Meier analysis for survival.
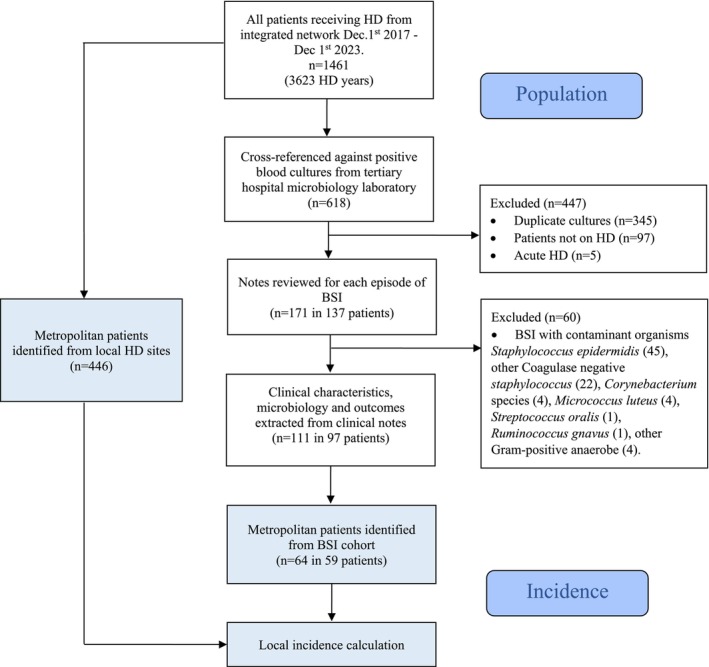
Results: Of 1461 patients who received HD over the study period, 171 positive blood cultures occurred in 137 patients. Sixty blood cultures (35%) were considered non-significant contaminants, leaving 111 significant BSIs in 97 patients. Patients with BSIs had a median age of 65 years (interquartile range [IQR]: 50-76); 61% were males, with 48% having diabetes mellitus and 57% cardiovascular disease. A high proportion of BSI episodes (66/111, 59%) were determined to be HD access-associated, primarily in patients with central venous catheters (55/111, 50%). The most frequent non-HD access-associated sources were intra-abdominal/biliary (9%) and urinary (8%). Staphylococcus aureus (25%) was the most isolated organism, followed by Staphylococcus epidermis (12%). Polymicrobial BSI occurred in 10% of episodes. Median hospitalisation length was 9 days (IQR: 6-15). Mortality at 90 days was high (24%), and on multivariate analysis was associated with increasing age (odds ratio: 1.06 per year [IQR: 1.01-1.10]).
Conclusion: BSIs remain a major issue in patients receiving HD, contributing to prolonged hospitalisations and high mortality rates. HD access-associated BSIs account for a substantial proportion of BSIs and remain a pertinent target for intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


