A retrospective study of the impact of comorbidity, polypharmacy and demographic factors on patient inclusion and healthcare delivery in phase I oncology trials.
Hoda Nemat, Martin Orr, Lucy Barrow, Bindu Raobaikady, Sheila Matharu, Lisa Scerri, Udai Banerji, Ceire Costelloe
{"title":"A retrospective study of the impact of comorbidity, polypharmacy and demographic factors on patient inclusion and healthcare delivery in phase I oncology trials.","authors":"Hoda Nemat, Martin Orr, Lucy Barrow, Bindu Raobaikady, Sheila Matharu, Lisa Scerri, Udai Banerji, Ceire Costelloe","doi":"10.1038/s44276-025-00165-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Phase I trials include patients with metastatic cancer and complex health conditions. Understanding baseline comorbidity and demographic features is critical to improving trial design.</p><p><strong>Methods: </strong>We used electronic patient records to study the association of comorbidity, polypharmacy, and demographic factors on trial recruitment, time on trial, and health service utilisation.</p><p><strong>Results: </strong>A cohort of 1671 patients was considered for allocation to a phase I study, of whom 518 patients were recruited to a phase I study and 1153 patients were not. A multivariable analysis revealed polypharmacy was associated with lower recruitment to phase I trials with an odds ratio of 0.95 (95% CI: [0.92, 0.99], p = 0.01), and a greater number of emergency admissions with a risk ratio of 1.1 (95% CI: [1.03, 1.17], p = 0.01). Interestingly, comorbidity was not associated with lower recruitment but was associated with a lower time on trial with a hazard ratio of 0.75 (95% CI: [0.62, 0.90], p ≤ 0.001). Demographic factors, including ethnicity, distance of residence from the hospital, and index of multiple deprivation, did not significantly influence these parameters.</p><p><strong>Conclusion: </strong>Polypharmacy and comorbidity should be considered both in the design of phase I oncology trials and in planning for healthcare utilisation during these trials.</p>","PeriodicalId":519964,"journal":{"name":"BJC reports","volume":"3 1","pages":"57"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12378352/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJC reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s44276-025-00165-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Phase I trials include patients with metastatic cancer and complex health conditions. Understanding baseline comorbidity and demographic features is critical to improving trial design.
Methods: We used electronic patient records to study the association of comorbidity, polypharmacy, and demographic factors on trial recruitment, time on trial, and health service utilisation.
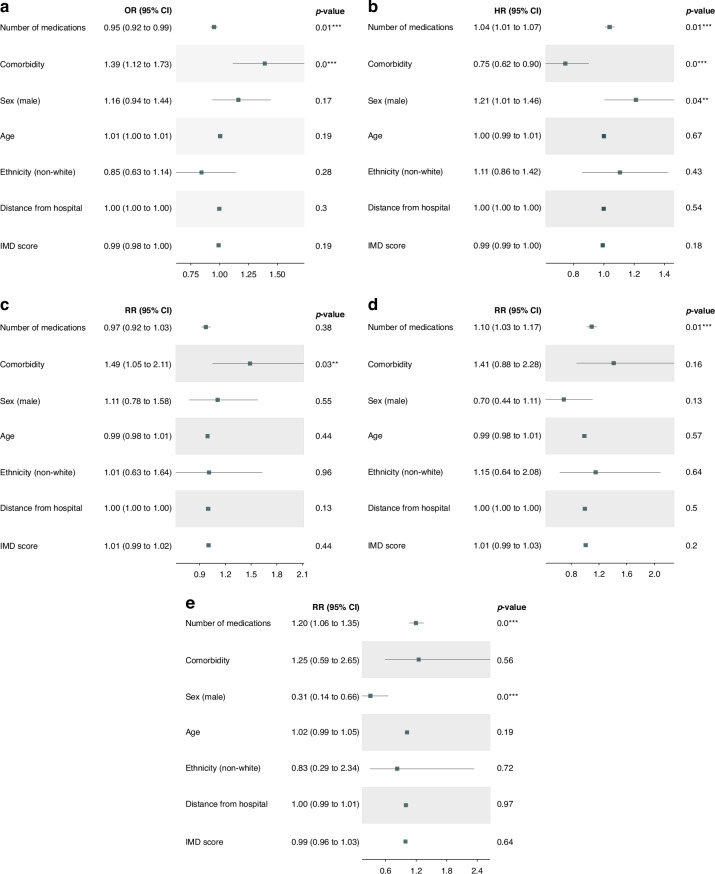
Results: A cohort of 1671 patients was considered for allocation to a phase I study, of whom 518 patients were recruited to a phase I study and 1153 patients were not. A multivariable analysis revealed polypharmacy was associated with lower recruitment to phase I trials with an odds ratio of 0.95 (95% CI: [0.92, 0.99], p = 0.01), and a greater number of emergency admissions with a risk ratio of 1.1 (95% CI: [1.03, 1.17], p = 0.01). Interestingly, comorbidity was not associated with lower recruitment but was associated with a lower time on trial with a hazard ratio of 0.75 (95% CI: [0.62, 0.90], p ≤ 0.001). Demographic factors, including ethnicity, distance of residence from the hospital, and index of multiple deprivation, did not significantly influence these parameters.
Conclusion: Polypharmacy and comorbidity should be considered both in the design of phase I oncology trials and in planning for healthcare utilisation during these trials.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


