{"title":"Device and surgical procedure-related infections in Canadian acute care hospitals, 2019-2023.","authors":"","doi":"10.14745/ccdr.v51i67a05","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Healthcare-associated infections (HAIs) are a significant healthcare burden in Canada. National surveillance of HAIs at sentinel acute care hospitals is conducted by the Canadian Nosocomial Infection Surveillance Program.</p><p><strong>Objective: </strong>This article describes device and surgical procedure-related HAI epidemiology in Canada from 2019 to 2023.</p><p><strong>Methods: </strong>Data were collected from 68 Canadian sentinel acute care hospitals between January 1, 2019, and December 31, 2023, for intensive care unit central line-associated bloodstream infections (ICU-CLABSIs), hip and knee surgical site infections (SSIs), cerebrospinal fluid (CSF) shunt SSIs and paediatric cardiac SSIs. Case counts, rates, patient and hospital characteristics, pathogen distributions and antimicrobial resistance data are presented.</p><p><strong>Results: </strong>Between 2019 and 2023, 2,582 device-related infections and 1,029 surgical procedure-related infections were reported. Rates of ICU-CLABSIs fluctuated throughout the study period, with an overall increase in all intensive care unit settings except for the neonatal intensive care unit, where a 4% decrease was noted. An increase in SSIs following knee arthroplasty was observed, rising from 0.34 to 0.43 infections per 100 surgeries. Fluctuating trends were also observed in CSF shunt SSIs and paediatric cardiac SSIs over the study period. The most commonly identified pathogens were coagulase-negative staphylococci (23%) in ICU-CLABSIs and <i>Staphylococcus aureus</i> (42%) in SSIs.</p><p><strong>Conclusion: </strong>Epidemiological and microbiological trends among selected device and surgical procedure-related HAIs are essential for benchmarking infection rates nationally and internationally, identifying any changes in infection rates or antimicrobial resistance patterns and helping inform hospital infection prevention and control and antimicrobial stewardship policies and programs.</p>","PeriodicalId":94304,"journal":{"name":"Canada communicable disease report = Releve des maladies transmissibles au Canada","volume":"51 6-7","pages":"270-283"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12373017/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canada communicable disease report = Releve des maladies transmissibles au Canada","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14745/ccdr.v51i67a05","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Healthcare-associated infections (HAIs) are a significant healthcare burden in Canada. National surveillance of HAIs at sentinel acute care hospitals is conducted by the Canadian Nosocomial Infection Surveillance Program.
Objective: This article describes device and surgical procedure-related HAI epidemiology in Canada from 2019 to 2023.
Methods: Data were collected from 68 Canadian sentinel acute care hospitals between January 1, 2019, and December 31, 2023, for intensive care unit central line-associated bloodstream infections (ICU-CLABSIs), hip and knee surgical site infections (SSIs), cerebrospinal fluid (CSF) shunt SSIs and paediatric cardiac SSIs. Case counts, rates, patient and hospital characteristics, pathogen distributions and antimicrobial resistance data are presented.
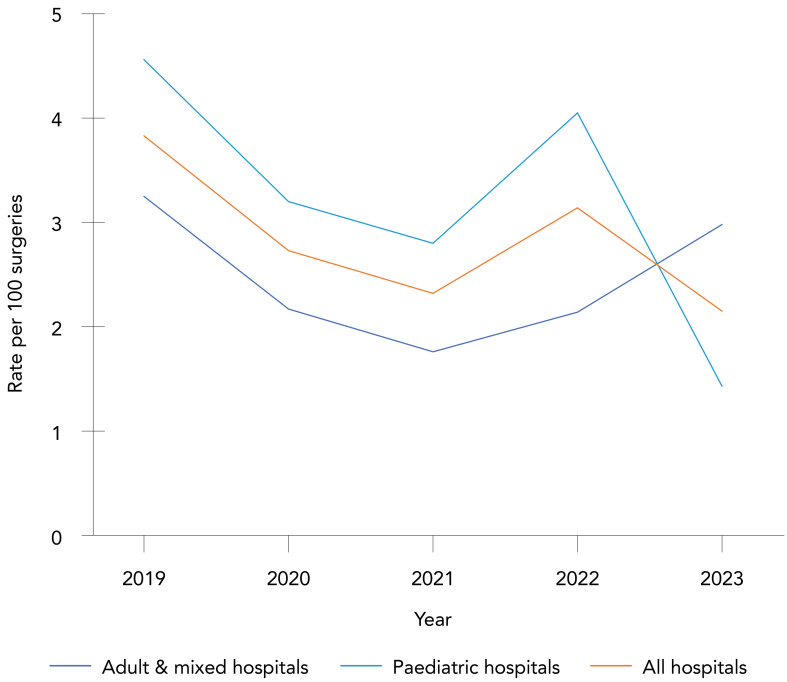
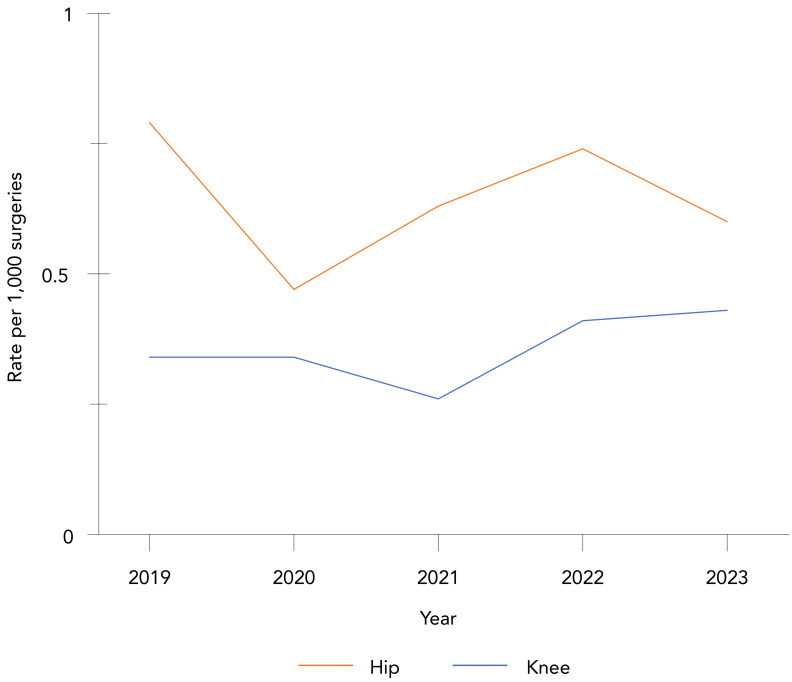
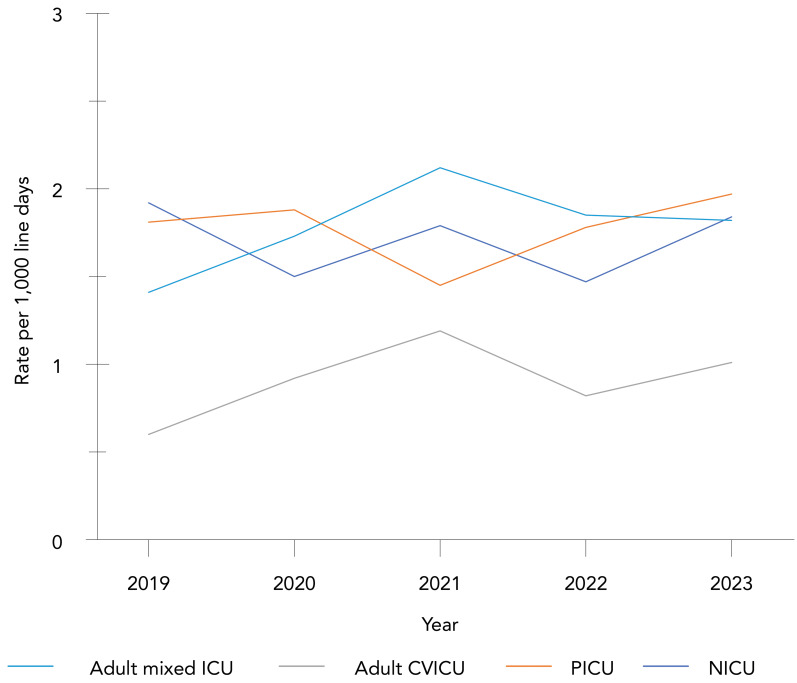
Results: Between 2019 and 2023, 2,582 device-related infections and 1,029 surgical procedure-related infections were reported. Rates of ICU-CLABSIs fluctuated throughout the study period, with an overall increase in all intensive care unit settings except for the neonatal intensive care unit, where a 4% decrease was noted. An increase in SSIs following knee arthroplasty was observed, rising from 0.34 to 0.43 infections per 100 surgeries. Fluctuating trends were also observed in CSF shunt SSIs and paediatric cardiac SSIs over the study period. The most commonly identified pathogens were coagulase-negative staphylococci (23%) in ICU-CLABSIs and Staphylococcus aureus (42%) in SSIs.
Conclusion: Epidemiological and microbiological trends among selected device and surgical procedure-related HAIs are essential for benchmarking infection rates nationally and internationally, identifying any changes in infection rates or antimicrobial resistance patterns and helping inform hospital infection prevention and control and antimicrobial stewardship policies and programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


