David K Ziayee, Ari D Kappel, David I Bass, Abdullah H Feroze, Sahin Hanalioglu, Neel Madan, Mohammad A Aziz-Sultan
{"title":"Percutaneous CT-guided Onyx embolization of CSF-venous fistula: illustrative case.","authors":"David K Ziayee, Ari D Kappel, David I Bass, Abdullah H Feroze, Sahin Hanalioglu, Neel Madan, Mohammad A Aziz-Sultan","doi":"10.3171/CASE2558","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>CSF-venous fistulas (CVFs) are an increasingly recognized cause of spontaneous intracranial hypotension (SIH). Cases of SIH can present with symptoms ranging from orthostatic headache to severe debilitating headaches, vertigo, back pain, vision changes, and cognitive impairment. CVFs are an aberrant direct fistulous connection between a spinal nerve root sleeve and adjacent paraspinal veins. Treatment options may include blood patch, surgical ligation, or transvenous embolization.</p><p><strong>Observations: </strong>A 67-year-old male presented with severe positional headaches following minor head trauma. MRI of the brain demonstrated pachymeningeal enhancement, and dynamic CT myelography demonstrated a CVF at the right T4 nerve root. Transvenous CVF embolization was attempted, but there was no suitable target for embolization despite extensive exploration of the azygos, paraspinal, and vertebral veins above and below the fistula. The patient underwent percutaneous puncture of the right T4 paraspinal vein using an 18-gauge Chiba needle under fluoroscopic guidance. Onyx 34 was carefully injected into the CVF under continuous fluoroscopic guidance to embolize the fistula and associated paraspinal venous complex.</p><p><strong>Lessons: </strong>In cases of challenging or difficult-to-access venous anatomy in which transvenous access to the fistulous site is not feasible, percutaneous needle puncture with direct transvenous embolization may be an option. https://thejns.org/doi/10.3171/CASE2558.</p>","PeriodicalId":94098,"journal":{"name":"Journal of neurosurgery. Case lessons","volume":"10 9","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400850/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of neurosurgery. Case lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE2558","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: CSF-venous fistulas (CVFs) are an increasingly recognized cause of spontaneous intracranial hypotension (SIH). Cases of SIH can present with symptoms ranging from orthostatic headache to severe debilitating headaches, vertigo, back pain, vision changes, and cognitive impairment. CVFs are an aberrant direct fistulous connection between a spinal nerve root sleeve and adjacent paraspinal veins. Treatment options may include blood patch, surgical ligation, or transvenous embolization.
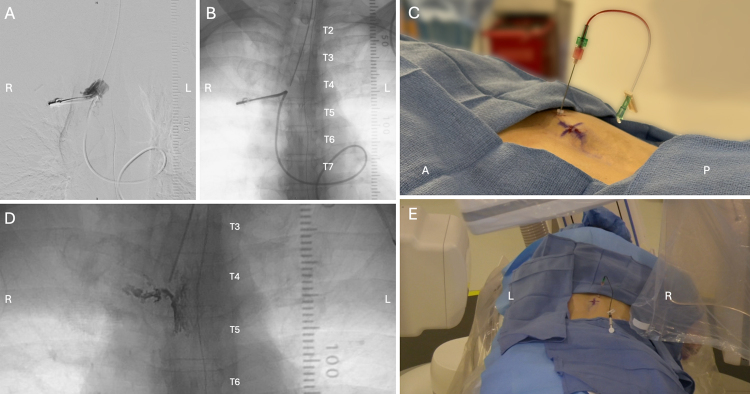
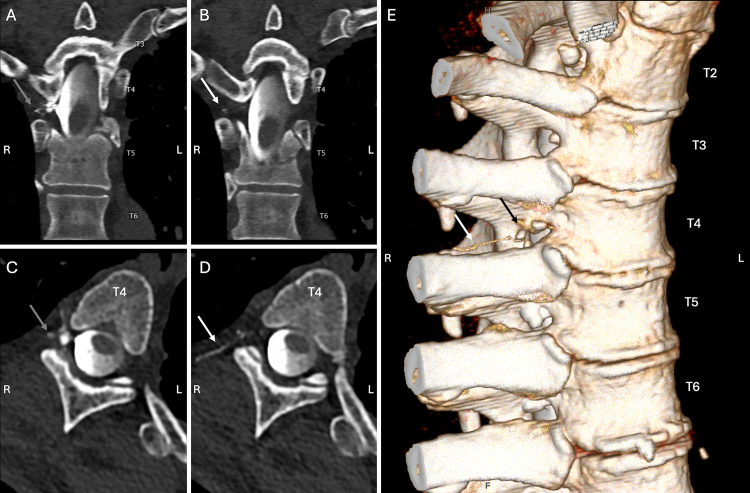
Observations: A 67-year-old male presented with severe positional headaches following minor head trauma. MRI of the brain demonstrated pachymeningeal enhancement, and dynamic CT myelography demonstrated a CVF at the right T4 nerve root. Transvenous CVF embolization was attempted, but there was no suitable target for embolization despite extensive exploration of the azygos, paraspinal, and vertebral veins above and below the fistula. The patient underwent percutaneous puncture of the right T4 paraspinal vein using an 18-gauge Chiba needle under fluoroscopic guidance. Onyx 34 was carefully injected into the CVF under continuous fluoroscopic guidance to embolize the fistula and associated paraspinal venous complex.
Lessons: In cases of challenging or difficult-to-access venous anatomy in which transvenous access to the fistulous site is not feasible, percutaneous needle puncture with direct transvenous embolization may be an option. https://thejns.org/doi/10.3171/CASE2558.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


