{"title":"Improving compliance to serum calcium and urate testing guidelines for patients with renal stones: a Two-Cycle audit.","authors":"Obinna Enemoh, Mayowa Adefehinti, Uchizi Mvalo, Obichukwu Iwunna","doi":"10.51894/001c.143427","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Renal stones develop when urinary solutes crystallize into solid deposits within the urinary tract. The 2019 National Institute for Health and Care Excellence (NICE) and British Association of Urological Surgeons (BAUS) guidelines recommend serum calcium and urate testing for all patients with renal or ureteric stones. This single-center audit aimed to assess compliance with these guidelines in a local urology department and implement quality improvement interventions to enhance adherence.</p><p><strong>Methods: </strong>We conducted a retrospective two-cycle audit on patients admitted with renal stones by the urology team at Chesterfield Royal Hospital, United Kingdom. Patient information and admission investigations were reviewed using the hospital's electronic medical records. Data were obtained from electronic medical records and assessed for compliance with calcium and urate testing guidelines. Interventions included educational sessions for clinicians, reminder posters, and updates to admission documentation. Pre- and post-intervention results were compared using statistical analysis.</p><p><strong>Results: </strong>A total of 70 patients were included (36 in the first cycle; 34 in the second). In the first cycle, urate testing was performed in 2 patients (5.6%), while calcium testing was performed in 31 (86.1%). Following the intervention, urate testing increased to 13 patients (38.2%; p = 0.00087) and calcium testing reached 100% compliance (p=0.0241).</p><p><strong>Conclusion: </strong>This audit identified poor adherence to urate and calcium testing guidelines for patients with renal stones. Educational and process interventions significantly improved compliance, achieving 100% for calcium testing and a more than sixfold increase in urate testing. Sustained improvement will require continued quality improvement measures.</p>","PeriodicalId":74853,"journal":{"name":"Spartan medical research journal","volume":"10 1","pages":"37-43"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392879/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spartan medical research journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.51894/001c.143427","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
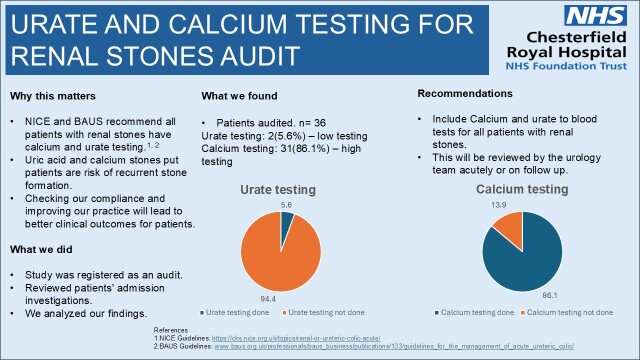
Introduction: Renal stones develop when urinary solutes crystallize into solid deposits within the urinary tract. The 2019 National Institute for Health and Care Excellence (NICE) and British Association of Urological Surgeons (BAUS) guidelines recommend serum calcium and urate testing for all patients with renal or ureteric stones. This single-center audit aimed to assess compliance with these guidelines in a local urology department and implement quality improvement interventions to enhance adherence.
Methods: We conducted a retrospective two-cycle audit on patients admitted with renal stones by the urology team at Chesterfield Royal Hospital, United Kingdom. Patient information and admission investigations were reviewed using the hospital's electronic medical records. Data were obtained from electronic medical records and assessed for compliance with calcium and urate testing guidelines. Interventions included educational sessions for clinicians, reminder posters, and updates to admission documentation. Pre- and post-intervention results were compared using statistical analysis.
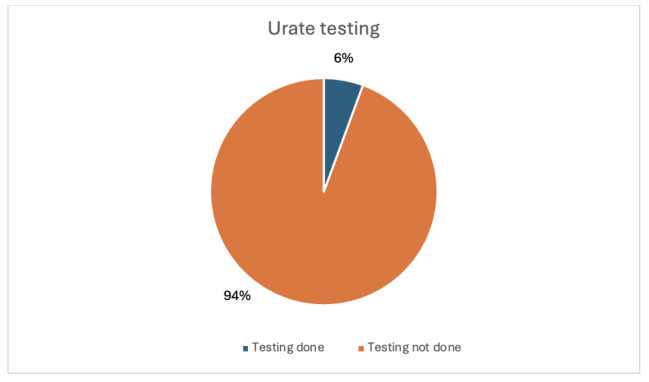
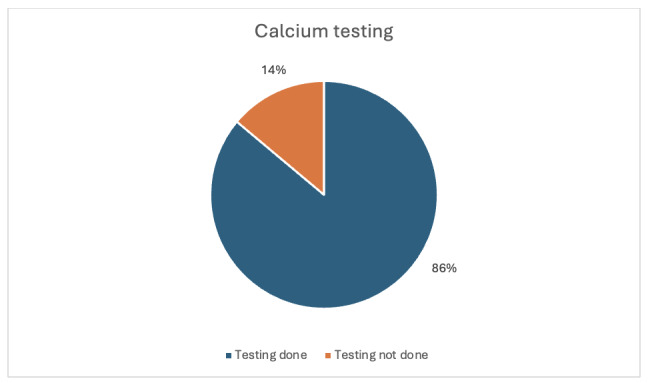
Results: A total of 70 patients were included (36 in the first cycle; 34 in the second). In the first cycle, urate testing was performed in 2 patients (5.6%), while calcium testing was performed in 31 (86.1%). Following the intervention, urate testing increased to 13 patients (38.2%; p = 0.00087) and calcium testing reached 100% compliance (p=0.0241).
Conclusion: This audit identified poor adherence to urate and calcium testing guidelines for patients with renal stones. Educational and process interventions significantly improved compliance, achieving 100% for calcium testing and a more than sixfold increase in urate testing. Sustained improvement will require continued quality improvement measures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


