Prognostic Factors and Clinical Outcomes of Spontaneous Intracerebral Hemorrhage: Analysis of 601 Consecutive Patients from a Single Center (2017-2023).
Cosmin Cindea, Vicentiu Saceleanu, Victor Tudor, Patrick Canning, Ovidiu Petrascu, Tamas Kerekes, Alexandru Breazu, Iulian Roman-Filip, Corina Roman-Filip, Romeo Mihaila
{"title":"Prognostic Factors and Clinical Outcomes of Spontaneous Intracerebral Hemorrhage: Analysis of 601 Consecutive Patients from a Single Center (2017-2023).","authors":"Cosmin Cindea, Vicentiu Saceleanu, Victor Tudor, Patrick Canning, Ovidiu Petrascu, Tamas Kerekes, Alexandru Breazu, Iulian Roman-Filip, Corina Roman-Filip, Romeo Mihaila","doi":"10.3390/neurosci6030077","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spontaneous intracerebral hemorrhage (ICH) has the highest case fatality of all stroke types, yet recent epidemiological and outcome data from Central and Eastern Europe remain limited.</p><p><strong>Methods: </strong>We retrospectively analyzed prospectively collected data for 601 consecutive adults with primary ICH admitted to Sibiu County Clinical Emergency Hospital, Romania (2017-2023). Demographics, Glasgow Coma Scale (GCS), CT-derived hematoma volume (ABC/2), anatomical site, intraventricular extension (IVH), treatment, comorbidities, and in-hospital death were reported with exact counts and percentages; no imputation was performed.</p><p><strong>Results: </strong>Mean age was 68.4 ± 12.9 years, and 59.7% were male. Mean hematoma volume was 30.4 mL, and 23.0% exceeded 30 mL. IVH occurred in 40.1% and doubled mortality (50.6% vs. 16.7%). Overall case fatality was 29.6% and climbed to 74.5% for brain-stem bleeds. Men, although younger than women (66.0 vs. 71.9 years), died more often (35.4% vs. 21.1%; risk ratio 1.67, 95% CI 1.26-2.21). Systemic hazards amplified death risk: Oral anticoagulation, 44.2%; chronic alcohol misuse, 51.4%; thrombocytopenia, 41.0%; chronic kidney disease, 42.3%. Conservative management (74.9%) yielded 27.8% mortality overall and ≤15 for small-to-mid lobar or capsulo-lenticular bleeds; lobar surgery matched this (13.4%) only in large clots. Thalamic evacuation was futile (82.3% mortality), and cerebellar decompression performed late still carried 54.5% mortality versus 16.6% medically. Multivariable analysis confirmed that low GCS, IVH, large hematoma volume, thrombocytopenia, and chronic alcohol use independently predicted in-hospital mortality.</p><p><strong>Limitations: </strong>This retrospective study lacked post-discharge functional outcome data (e.g., mRS at 90 days).</p><p><strong>Conclusions: </strong>This study presents the largest Romanian single-center ICH cohort, establishing national benchmarks and underscoring modifiable risk factors. Early ICH lethality aligns with Western data but is amplified by exposures such as alcohol misuse, anticoagulation, thrombocytopenia, and CKD. Priorities include preventive strategies, timely surgical access, wider adoption of minimally invasive techniques, and development of a prospective regional registry.</p>","PeriodicalId":74294,"journal":{"name":"NeuroSci","volume":"6 3","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2025-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372121/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"NeuroSci","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurosci6030077","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Spontaneous intracerebral hemorrhage (ICH) has the highest case fatality of all stroke types, yet recent epidemiological and outcome data from Central and Eastern Europe remain limited.
Methods: We retrospectively analyzed prospectively collected data for 601 consecutive adults with primary ICH admitted to Sibiu County Clinical Emergency Hospital, Romania (2017-2023). Demographics, Glasgow Coma Scale (GCS), CT-derived hematoma volume (ABC/2), anatomical site, intraventricular extension (IVH), treatment, comorbidities, and in-hospital death were reported with exact counts and percentages; no imputation was performed.
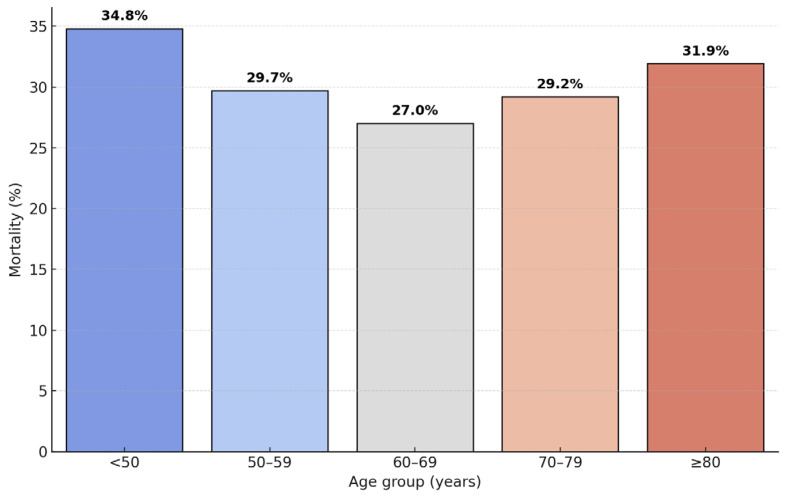
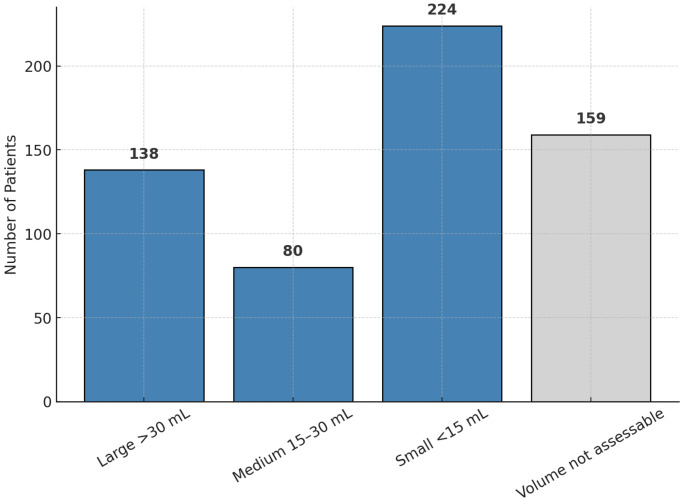
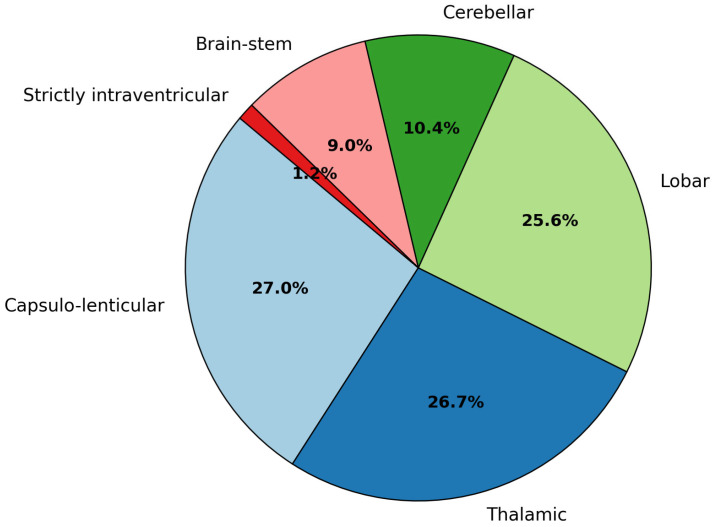
Results: Mean age was 68.4 ± 12.9 years, and 59.7% were male. Mean hematoma volume was 30.4 mL, and 23.0% exceeded 30 mL. IVH occurred in 40.1% and doubled mortality (50.6% vs. 16.7%). Overall case fatality was 29.6% and climbed to 74.5% for brain-stem bleeds. Men, although younger than women (66.0 vs. 71.9 years), died more often (35.4% vs. 21.1%; risk ratio 1.67, 95% CI 1.26-2.21). Systemic hazards amplified death risk: Oral anticoagulation, 44.2%; chronic alcohol misuse, 51.4%; thrombocytopenia, 41.0%; chronic kidney disease, 42.3%. Conservative management (74.9%) yielded 27.8% mortality overall and ≤15 for small-to-mid lobar or capsulo-lenticular bleeds; lobar surgery matched this (13.4%) only in large clots. Thalamic evacuation was futile (82.3% mortality), and cerebellar decompression performed late still carried 54.5% mortality versus 16.6% medically. Multivariable analysis confirmed that low GCS, IVH, large hematoma volume, thrombocytopenia, and chronic alcohol use independently predicted in-hospital mortality.
Limitations: This retrospective study lacked post-discharge functional outcome data (e.g., mRS at 90 days).
Conclusions: This study presents the largest Romanian single-center ICH cohort, establishing national benchmarks and underscoring modifiable risk factors. Early ICH lethality aligns with Western data but is amplified by exposures such as alcohol misuse, anticoagulation, thrombocytopenia, and CKD. Priorities include preventive strategies, timely surgical access, wider adoption of minimally invasive techniques, and development of a prospective regional registry.
背景:自发性脑出血(ICH)是所有脑卒中类型中病死率最高的,但最近来自中欧和东欧的流行病学和结局数据仍然有限。方法:回顾性分析罗马尼亚锡比乌县临床急救医院(Sibiu County Clinical Emergency Hospital, Romania, 2017-2023) 601例原发性脑出血连续成人患者的前瞻性数据。统计数据、格拉斯哥昏迷量表(GCS)、ct血肿体积(ABC/2)、解剖部位、脑室内延伸(IVH)、治疗、合并症和院内死亡报告了确切的计数和百分比;未进行imputation。结果:平均年龄68.4±12.9岁,男性占59.7%。平均血肿体积为30.4 mL, 23.0%超过30 mL。IVH发生率为40.1%,死亡率翻倍(50.6% vs. 16.7%)。总病死率为29.6%,脑干出血病死率攀升至74.5%。男性虽然比女性年轻(66.0岁比71.9岁),但死亡频率更高(35.4%比21.1%;风险比1.67,95% CI 1.26-2.21)。系统性危险放大死亡风险:口服抗凝剂,44.2%;慢性酒精滥用,51.4%;血小板减少症,41.0%;慢性肾脏疾病,42.3%。保守治疗(74.9%)的总死亡率为27.8%,小到中叶或囊状透镜出血的死亡率≤15;大叶手术仅在大血块中与此相符(13.4%)。丘脑引流无效(死亡率82.3%),晚行小脑减压仍有54.5%的死亡率,而医学上的死亡率为16.6%。多变量分析证实,低GCS、IVH、大血肿量、血小板减少和慢性酒精使用独立预测院内死亡率。局限性:本回顾性研究缺乏出院后功能结局数据(如90天mRS)。结论:本研究是罗马尼亚最大的单中心ICH队列研究,建立了国家基准,并强调了可改变的危险因素。早期脑出血致死率与西方数据一致,但由于酒精滥用、抗凝、血小板减少症和慢性肾病等暴露而被放大。优先事项包括预防策略、及时手术、更广泛地采用微创技术以及发展前瞻性区域登记。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


