Stefanie Stramel-Stafford, Heather Townsend, Brian Trimmer, James Cohen, Jessica Thompson
{"title":"Evaluation of a Febrile Neutropenia Protocol Implemented at Triage in an Emergency Department.","authors":"Stefanie Stramel-Stafford, Heather Townsend, Brian Trimmer, James Cohen, Jessica Thompson","doi":"10.3390/medicines12030020","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective:</b> The impact of a febrile neutropenia (FN) emergency department (ED) triage screening tool and protocol on time to antibiotic administration (TTA) and patient outcomes was evaluated. <b>Methods:</b> This was a retrospective, quasi-experimental study of adult FN patients admitted through the ED from April 2014 to April 2017. In March 2016 a triage screening tool and protocol were implemented. In patients who screened positive, nursing initiated a protocol that included laboratory diagnostics and a pharmacy consult for empiric antibiotics prior to evaluation by a provider. Patients were evaluated pre- and post-protocol for TTA, 30-day mortality, ED length of stay (LOS), and hospital LOS. <b>Results:</b> A total of 130 patients were included in the study, 77 pre-protocol and 53 post-protocol. Median TTA was longer in the pre-protocol group at 174 min (interquartile range [IQR] 105-224) vs. 109 min (IQR 71-214) post-protocol, <i>p</i> = 0.04. Thirty-day mortality was greater at 18.8% pre-protocol vs. 7.5% post-protocol, <i>p</i> = 0.12. There was no difference in hospital LOS. Pre-protocol patients compared to post-protocol patients who had a pharmacy consult demonstrated a further reduction in TTA (174 min [IQR 105-224] vs. 87.5 min [IQR 61.5-135], <i>p</i> < 0.01) and a reduced mortality (18% vs. 0%, <i>p</i> = 0.04). <b>Conclusions:</b> To our knowledge, this is the first report of a protocol for febrile neutropenia that allows pharmacists to order antibiotics based on a nurse triage assessment. Evaluation of the protocol demonstrated a significant reduction in TTA and trend toward improved mortality.</p>","PeriodicalId":74162,"journal":{"name":"Medicines (Basel, Switzerland)","volume":"12 3","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372115/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medicines (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/medicines12030020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
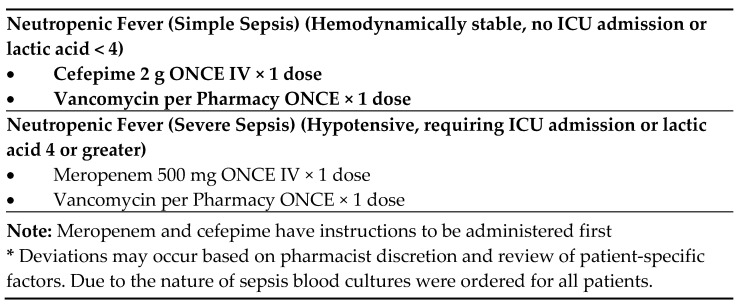
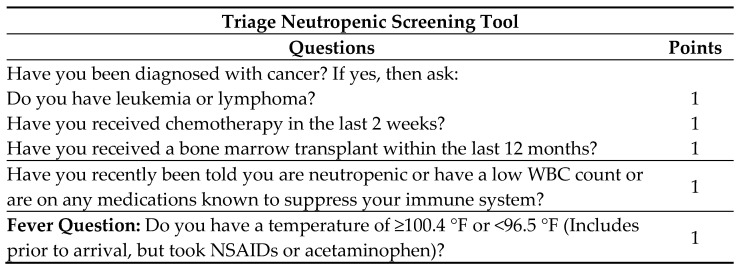
Objective: The impact of a febrile neutropenia (FN) emergency department (ED) triage screening tool and protocol on time to antibiotic administration (TTA) and patient outcomes was evaluated. Methods: This was a retrospective, quasi-experimental study of adult FN patients admitted through the ED from April 2014 to April 2017. In March 2016 a triage screening tool and protocol were implemented. In patients who screened positive, nursing initiated a protocol that included laboratory diagnostics and a pharmacy consult for empiric antibiotics prior to evaluation by a provider. Patients were evaluated pre- and post-protocol for TTA, 30-day mortality, ED length of stay (LOS), and hospital LOS. Results: A total of 130 patients were included in the study, 77 pre-protocol and 53 post-protocol. Median TTA was longer in the pre-protocol group at 174 min (interquartile range [IQR] 105-224) vs. 109 min (IQR 71-214) post-protocol, p = 0.04. Thirty-day mortality was greater at 18.8% pre-protocol vs. 7.5% post-protocol, p = 0.12. There was no difference in hospital LOS. Pre-protocol patients compared to post-protocol patients who had a pharmacy consult demonstrated a further reduction in TTA (174 min [IQR 105-224] vs. 87.5 min [IQR 61.5-135], p < 0.01) and a reduced mortality (18% vs. 0%, p = 0.04). Conclusions: To our knowledge, this is the first report of a protocol for febrile neutropenia that allows pharmacists to order antibiotics based on a nurse triage assessment. Evaluation of the protocol demonstrated a significant reduction in TTA and trend toward improved mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


