Comparative study of modified midline lumbar interbody fusion and modified transforaminal lumbar interbody fusion for the treatment of single-level lumbar degenerative diseases.
{"title":"Comparative study of modified midline lumbar interbody fusion and modified transforaminal lumbar interbody fusion for the treatment of single-level lumbar degenerative diseases.","authors":"Yuanpeng Yue, Yihui Liu, Ce Dong, Zhenyu Wang","doi":"10.1186/s12893-025-03100-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To evaluate the safety and efficacy of modified cortical bone trajectory (MCBT) screw combined with transarticular screw (TASS) fixation (MCBT-TASS) in modified midline lumbar interbody fusion (M-MIDLIF) for single-level lumbar degenerative disease (LDD).</p><p><strong>Methods: </strong>We retrospectively included 104 patients with L4-5 or L5-S1 single-segment LDD who had indications for decompression, fusion, and internal fixation surgery from 2019 to 2022. They were subsequently divided into M-MIDLIF and modified transforaminal lumbar interbody fusion (M-TLIF) groups according to the surgical approach. Basic demographic, surgical, and radiological data, as well as clinical outcomes (Oswestry Disability Index (ODI) and visual analog scale (VAS) scores), were collected.</p><p><strong>Results: </strong>Basic demographic data, fusion rates, postoperative hospital stays, and follow-up times did not significantly differ between the two groups. Compared with those in the M-TLIF group, the intraoperative blood loss (68.57 ± 14.84 mL) and postoperative drainage volume (33.93 ± 9.17 mL) in the M-MIDLIF group were lower (intraoperative blood loss: 171.79 ± 12.78 mL, p < 0.05; postoperative drainage volume: 65.36 ± 10.36, p < 0.05). In the M-MIDLIF group, there was no significant difference in the radiographic recognizable rate (91.07%) or intraoperative visual recognizable rate (87.50%) of internal inverted chevron-shaped (V-shaped) crests. The optimal position screw rates for the MCBT, TASS, and traditional pedicle screw (TPS) methods were 94.64%, 94.64%, and 87.5%, respectively, and the differences were not significant. MCBT technology preserved the integrity of the posterior ligamentous complex (PLC) in 92.85% of patients in the M-MIDLIF group. The facet joint violation (FJV) rate of MCBT screws (3.57%) was lower than that of TPS screws (14.29%). Compared with the M-TLIF group, the M-MIDLIF group presented greater reductions in the ODI and VAS scores for both low back and leg pain at 1 week postoperatively (P < 0.05). However, no statistically significant differences in these scores were observed between the two groups at later time points (p > 0.05).</p><p><strong>Conclusion: </strong>M-MIDLIF can achieve decompression, fixation, and fusion via a median incision while preserving the integrity of the posterior ligamentous complex. In the treatment of single-level lumbar degenerative disease, M-MIDLIF has comparatively enhanced minimally invasive advantages over M-TLIF during the perioperative period while maintaining non-inferior clinical safety and efficacy relative to M-TLIF.</p>","PeriodicalId":49229,"journal":{"name":"BMC Surgery","volume":"25 1","pages":"384"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372285/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12893-025-03100-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To evaluate the safety and efficacy of modified cortical bone trajectory (MCBT) screw combined with transarticular screw (TASS) fixation (MCBT-TASS) in modified midline lumbar interbody fusion (M-MIDLIF) for single-level lumbar degenerative disease (LDD).
Methods: We retrospectively included 104 patients with L4-5 or L5-S1 single-segment LDD who had indications for decompression, fusion, and internal fixation surgery from 2019 to 2022. They were subsequently divided into M-MIDLIF and modified transforaminal lumbar interbody fusion (M-TLIF) groups according to the surgical approach. Basic demographic, surgical, and radiological data, as well as clinical outcomes (Oswestry Disability Index (ODI) and visual analog scale (VAS) scores), were collected.
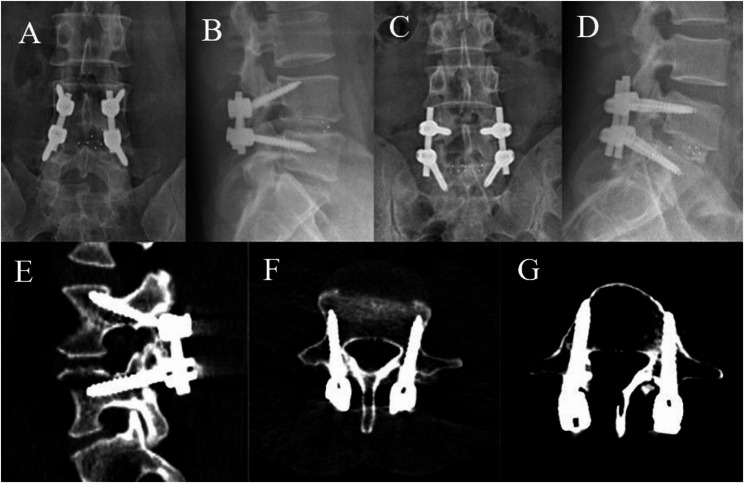
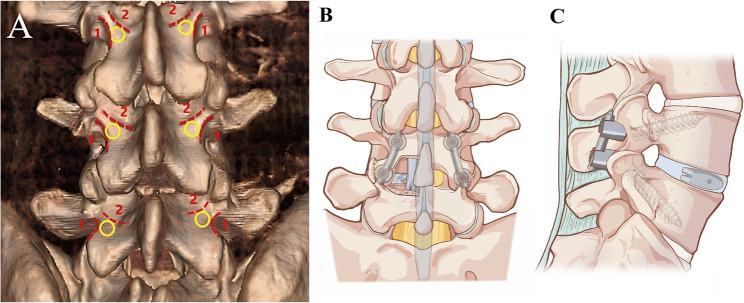
Results: Basic demographic data, fusion rates, postoperative hospital stays, and follow-up times did not significantly differ between the two groups. Compared with those in the M-TLIF group, the intraoperative blood loss (68.57 ± 14.84 mL) and postoperative drainage volume (33.93 ± 9.17 mL) in the M-MIDLIF group were lower (intraoperative blood loss: 171.79 ± 12.78 mL, p < 0.05; postoperative drainage volume: 65.36 ± 10.36, p < 0.05). In the M-MIDLIF group, there was no significant difference in the radiographic recognizable rate (91.07%) or intraoperative visual recognizable rate (87.50%) of internal inverted chevron-shaped (V-shaped) crests. The optimal position screw rates for the MCBT, TASS, and traditional pedicle screw (TPS) methods were 94.64%, 94.64%, and 87.5%, respectively, and the differences were not significant. MCBT technology preserved the integrity of the posterior ligamentous complex (PLC) in 92.85% of patients in the M-MIDLIF group. The facet joint violation (FJV) rate of MCBT screws (3.57%) was lower than that of TPS screws (14.29%). Compared with the M-TLIF group, the M-MIDLIF group presented greater reductions in the ODI and VAS scores for both low back and leg pain at 1 week postoperatively (P < 0.05). However, no statistically significant differences in these scores were observed between the two groups at later time points (p > 0.05).
Conclusion: M-MIDLIF can achieve decompression, fixation, and fusion via a median incision while preserving the integrity of the posterior ligamentous complex. In the treatment of single-level lumbar degenerative disease, M-MIDLIF has comparatively enhanced minimally invasive advantages over M-TLIF during the perioperative period while maintaining non-inferior clinical safety and efficacy relative to M-TLIF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


