Wei-Zhen Tang, Kang-Jin Huang, Xia Li, Qin-Yu Cai, Ying-Xiong Wang, Hong-Yu Xu, Li Wen, Lan Wang, Tai-Hang Liu
{"title":"Differential risk and clinical characteristics of placenta accreta spectrum in twin and singleton pregnancies: implications for perinatal outcomes.","authors":"Wei-Zhen Tang, Kang-Jin Huang, Xia Li, Qin-Yu Cai, Ying-Xiong Wang, Hong-Yu Xu, Li Wen, Lan Wang, Tai-Hang Liu","doi":"10.7189/jogh.15.04252","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study compares the prevalence of placenta accreta in singleton and twin pregnancies and examines its impact on adverse perinatal outcomes, exploring whether twin gestation increases the risk of poor outcomes in placenta accreta cases.</p><p><strong>Methods: </strong>A multivariate logistic regression analysis assessed the link between twin pregnancy and placenta accreta, comparing associated adverse perinatal outcomes in twin vs. singleton pregnancies. Stratified and interaction analyses explored clinical characteristics' relationship with placenta accreta. The Restrictive Cubic Spline (RCS) model evaluated the impact of placenta accreta on caesarean section and postpartum haemorrhage at different gestational ages. A comparative analysis examined clinical features and perinatal outcomes between twin and singleton pregnancies with placenta accreta. Finally, mediation analysis was used to determine if placenta accreta mediates the effect of twin gestation on caesarean section and postpartum haemorrhage.</p><p><strong>Results: </strong>In a large cohort study of 16 908 pregnancies, including both twin and singleton pregnancies, conducted in Chongqing, China, the risk of placenta accreta increased by 51% in twin gestations, with haemorrhagic placenta accreta rising by 133%. This condition significantly heightened the risk of adverse perinatal outcomes in both singleton and twin pregnancies, with twin pregnancies exhibiting higher risks. In twins, the risk of preterm birth was 1.77 (95% confidence interval (CI) = 1.24, 2.52), caesarean section was 4.87 (95% CI = 3.00, 7.90), postpartum haemorrhage was 3.73 (95% CI = 1.95, 7.13), and uterine rupture was 26.42 (95% CI = 2.28, 306.63). Additionally, placenta accreta showed different interactions with various factors in both twin and singleton pregnancies, influencing distinct outcomes. Restricted Cubic Splines (RCS) model analysis indicated an increasing trend in the risk of caesarean section and postpartum haemorrhage associated with placenta accreta across all gestational ages in both singleton and twin gestations. In patients with placenta accreta, the risks of preterm birth, caesarean section, pelvic inflammatory disease, atonic postpartum haemorrhage, and premature rupture of membranes in twin gestations were 6.77, 2.39, 2.54, 5.84, and 2.93 times higher, respectively, than in singleton gestations. Finally, mediation causal analysis revealed that the effect of twin gestation on caesarean section included both a direct effect and an indirect effect mediated through placenta accreta. For postpartum haemorrhage, the effect of twin gestation was mediated through placenta accreta.</p><p><strong>Conclusions: </strong>Twin gestation, regardless of known risk factors, increases the risk of placenta accreta and adverse perinatal outcomes compared to singleton pregnancies. Antenatal interventions and delivery risk management are essential for twin pregnancies with placenta accreta.</p>","PeriodicalId":48734,"journal":{"name":"Journal of Global Health","volume":"15 ","pages":"04252"},"PeriodicalIF":4.3000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12371300/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Global Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.7189/jogh.15.04252","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study compares the prevalence of placenta accreta in singleton and twin pregnancies and examines its impact on adverse perinatal outcomes, exploring whether twin gestation increases the risk of poor outcomes in placenta accreta cases.
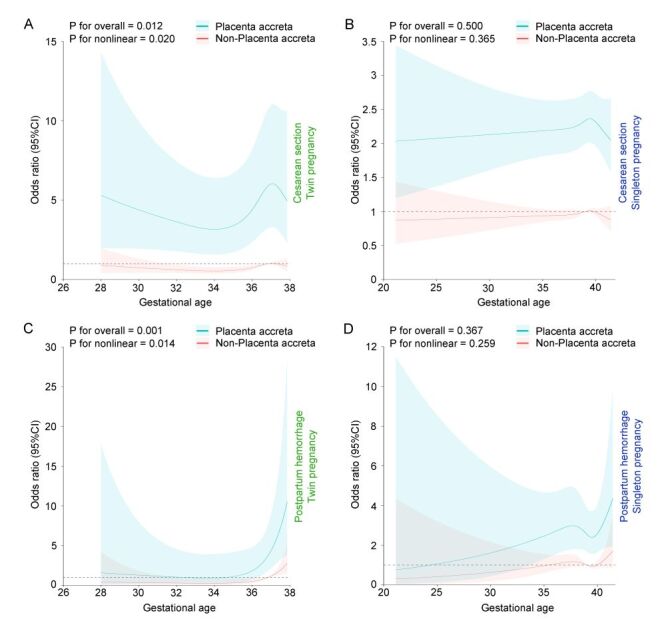
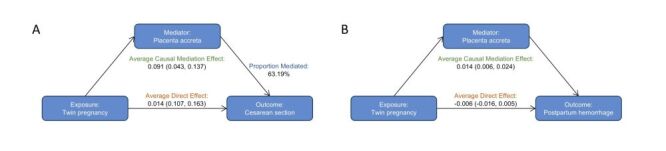
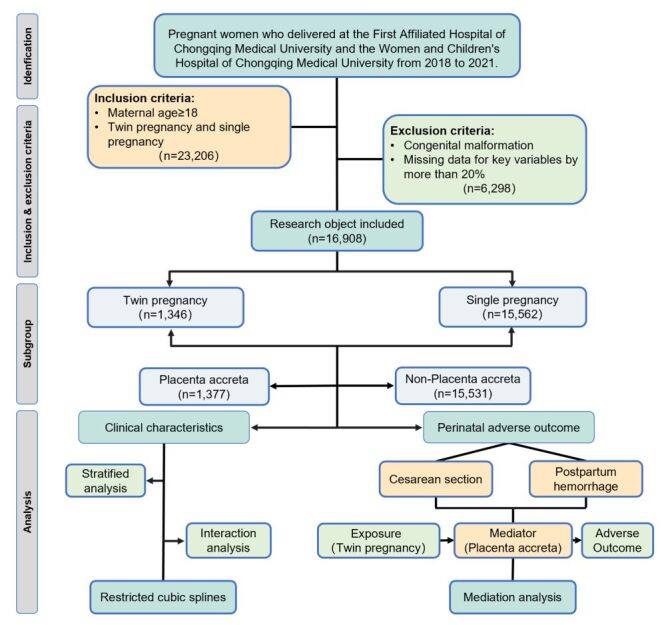
Methods: A multivariate logistic regression analysis assessed the link between twin pregnancy and placenta accreta, comparing associated adverse perinatal outcomes in twin vs. singleton pregnancies. Stratified and interaction analyses explored clinical characteristics' relationship with placenta accreta. The Restrictive Cubic Spline (RCS) model evaluated the impact of placenta accreta on caesarean section and postpartum haemorrhage at different gestational ages. A comparative analysis examined clinical features and perinatal outcomes between twin and singleton pregnancies with placenta accreta. Finally, mediation analysis was used to determine if placenta accreta mediates the effect of twin gestation on caesarean section and postpartum haemorrhage.
Results: In a large cohort study of 16 908 pregnancies, including both twin and singleton pregnancies, conducted in Chongqing, China, the risk of placenta accreta increased by 51% in twin gestations, with haemorrhagic placenta accreta rising by 133%. This condition significantly heightened the risk of adverse perinatal outcomes in both singleton and twin pregnancies, with twin pregnancies exhibiting higher risks. In twins, the risk of preterm birth was 1.77 (95% confidence interval (CI) = 1.24, 2.52), caesarean section was 4.87 (95% CI = 3.00, 7.90), postpartum haemorrhage was 3.73 (95% CI = 1.95, 7.13), and uterine rupture was 26.42 (95% CI = 2.28, 306.63). Additionally, placenta accreta showed different interactions with various factors in both twin and singleton pregnancies, influencing distinct outcomes. Restricted Cubic Splines (RCS) model analysis indicated an increasing trend in the risk of caesarean section and postpartum haemorrhage associated with placenta accreta across all gestational ages in both singleton and twin gestations. In patients with placenta accreta, the risks of preterm birth, caesarean section, pelvic inflammatory disease, atonic postpartum haemorrhage, and premature rupture of membranes in twin gestations were 6.77, 2.39, 2.54, 5.84, and 2.93 times higher, respectively, than in singleton gestations. Finally, mediation causal analysis revealed that the effect of twin gestation on caesarean section included both a direct effect and an indirect effect mediated through placenta accreta. For postpartum haemorrhage, the effect of twin gestation was mediated through placenta accreta.
Conclusions: Twin gestation, regardless of known risk factors, increases the risk of placenta accreta and adverse perinatal outcomes compared to singleton pregnancies. Antenatal interventions and delivery risk management are essential for twin pregnancies with placenta accreta.
期刊介绍:
Journal of Global Health is a peer-reviewed journal published by the Edinburgh University Global Health Society, a not-for-profit organization registered in the UK. We publish editorials, news, viewpoints, original research and review articles in two issues per year.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


