{"title":"Nurse Perspectives on Prone Positioning for ARDS Patient in the ICU: A Qualitative Phenomenological Study of Facilitator and Barrier.","authors":"Sriyono Sriyono, Hakim Zulkarnain, Erna Dwi Wahyuni, Jujuk Proboningsih, Wikan Purwihantoro, Maria-Pilar Mosteiro-Diaz","doi":"10.1177/23779608251371102","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Prone positioning is an established therapeutic intervention for acute respiratory distress syndrome (ARDS) patients. However, its utilization in ARDS treatment remains low, despite recommendations and evidence of its benefits.</p><p><strong>Objective: </strong>This study aims to explore the phenomenon of performing prone position for ARDS patients in the intensive care unit (ICU), especially from the nurses' perspective of the facilitators and the barrier.</p><p><strong>Methods: </strong>A qualitative phenomenological approach was employed. Fifteen ICU nurses from a referral hospital in Surabaya, Indonesia, who had performed at least 10 prone positions on intubated patients, were interviewed. Thematic analysis was conducted to identify emerging themes.</p><p><strong>Results: </strong>The facilitator factors are the availability of specially designed tool, the knowledge about benefit for the patient, and the availability of plan to mitigate complication. The barrier factors are the heavy maneuver during the process, the needs of lots of manpower, and the agitating patient. The facilitators lead the nurse to following way, the availability of specialized design tools enhances nurse confidence and patient safety. Then, the knowledge related to prone positioning benefit reinforced prone position importance. Additionally, a planning and proactive measures are necessary since the prone positioning is posed risk. The barrier holds the nurse performance in the following way: the physical demand may lead to musculoskeletal problems, such as back pain; inadequate staffing results in procedure delays or cancellations. Patient agitation, especially in intubated and mechanically ventilated patients, posed additional challenges, including the risk of extubating and increased congestion.</p><p><strong>Conclusion: </strong>ICU setting needs to be supportive to promote safe and effective prone positioning practices. This can be achieved through addressing the facilitator and the barrier of prone position. Additionally, prone positioning guideline development should involve the nurse.</p>","PeriodicalId":43312,"journal":{"name":"SAGE Open Nursing","volume":"11 ","pages":"23779608251371102"},"PeriodicalIF":2.5000,"publicationDate":"2025-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12378304/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Nursing","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23779608251371102","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"NURSING","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Prone positioning is an established therapeutic intervention for acute respiratory distress syndrome (ARDS) patients. However, its utilization in ARDS treatment remains low, despite recommendations and evidence of its benefits.
Objective: This study aims to explore the phenomenon of performing prone position for ARDS patients in the intensive care unit (ICU), especially from the nurses' perspective of the facilitators and the barrier.
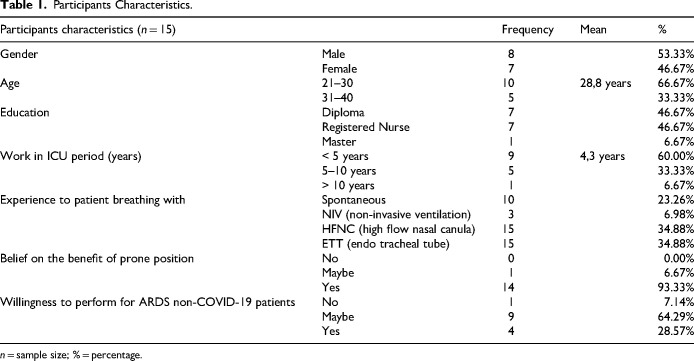
Methods: A qualitative phenomenological approach was employed. Fifteen ICU nurses from a referral hospital in Surabaya, Indonesia, who had performed at least 10 prone positions on intubated patients, were interviewed. Thematic analysis was conducted to identify emerging themes.
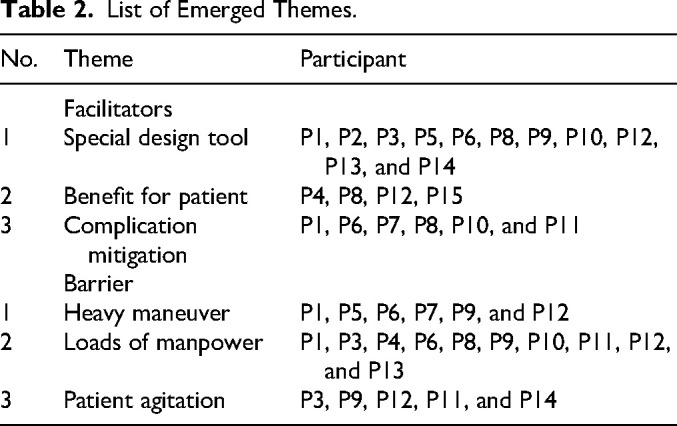
Results: The facilitator factors are the availability of specially designed tool, the knowledge about benefit for the patient, and the availability of plan to mitigate complication. The barrier factors are the heavy maneuver during the process, the needs of lots of manpower, and the agitating patient. The facilitators lead the nurse to following way, the availability of specialized design tools enhances nurse confidence and patient safety. Then, the knowledge related to prone positioning benefit reinforced prone position importance. Additionally, a planning and proactive measures are necessary since the prone positioning is posed risk. The barrier holds the nurse performance in the following way: the physical demand may lead to musculoskeletal problems, such as back pain; inadequate staffing results in procedure delays or cancellations. Patient agitation, especially in intubated and mechanically ventilated patients, posed additional challenges, including the risk of extubating and increased congestion.
Conclusion: ICU setting needs to be supportive to promote safe and effective prone positioning practices. This can be achieved through addressing the facilitator and the barrier of prone position. Additionally, prone positioning guideline development should involve the nurse.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


