Yan Efrata Sembiring, Fan Maitri Aldian, Amy Rosalie Sukamto
{"title":"Air Rifle Injury: Rare Bullet Lodgement in the Right Ventricle and Successful Surgical Removal.","authors":"Yan Efrata Sembiring, Fan Maitri Aldian, Amy Rosalie Sukamto","doi":"10.12659/AJCR.948109","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Air rifles, frequently used in sports, can cause complex, violent, and traumatic cardiac injury associated with significant morbidity and mortality. Unlike firearm projectiles, air rifle pellets lack rotational movement but can achieve velocities of 100 to 230 m/s. CASE REPORT A 21-year-old man was referred to our hospital after sustaining an air rifle injury to the right chest. He presented 10 h after injury with chest pain but was hemodynamically stable. Physical examination revealed decreased breath sounds and tenderness in the right hemithorax. Chest X-ray showed right-sided hemothorax and pulmonary contusion, prompting chest tube placement, with initial drainage of 500 cc hemorrhagic fluid. Transthoracic echocardiography identified a hyperechoic mass in the right ventricle, with mild pericardial effusion. Computed tomography confirmed the projectile was lodged in the posterior right ventricle, 0.8 cm from the tricuspid annulus. Emergency surgery was performed and successfully extracted an intact 3×3×5 mm air gun pellet. Postoperatively, the patient experienced a brief tonic-clonic seizure, which was managed with midazolam and propofol. He received prophylactic ceftriaxone, intravenous phenytoin, vitamin B6, and folic acid and oral aspirin, ibuprofen, and omeprazole. The patient showed improvement by postoperative day 3 and was discharged on day 4. Weekly follow-ups and an EEG 1 month after discharge showed normal results. At the 2-month follow-up, the patient remained asymptomatic. CONCLUSIONS Awareness of cardiac penetrating wounds, bullet trajectory, and clinical signs, along with a multidisciplinary approach and patient-family involvement, is crucial for favorable outcomes and long-term follow-up.</p>","PeriodicalId":39064,"journal":{"name":"American Journal of Case Reports","volume":"26 ","pages":"e948109"},"PeriodicalIF":0.7000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404002/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.948109","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
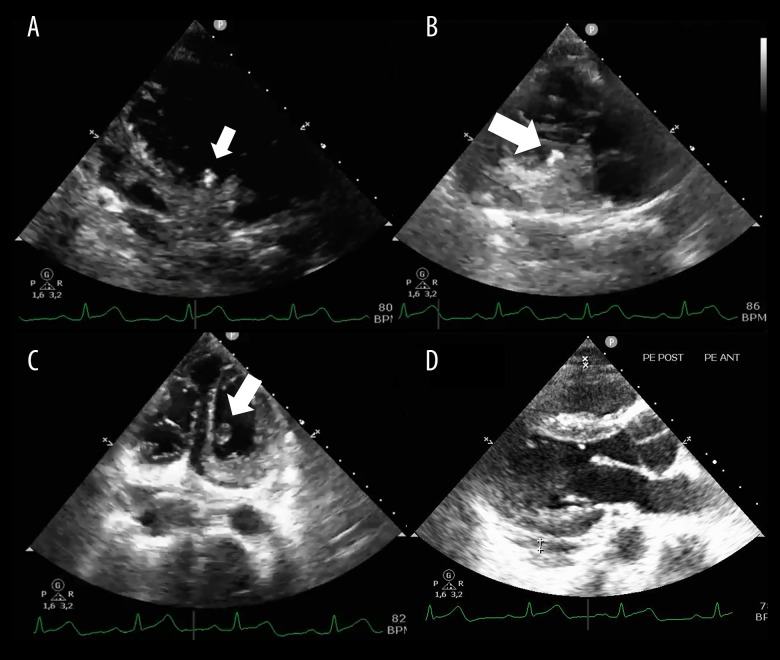
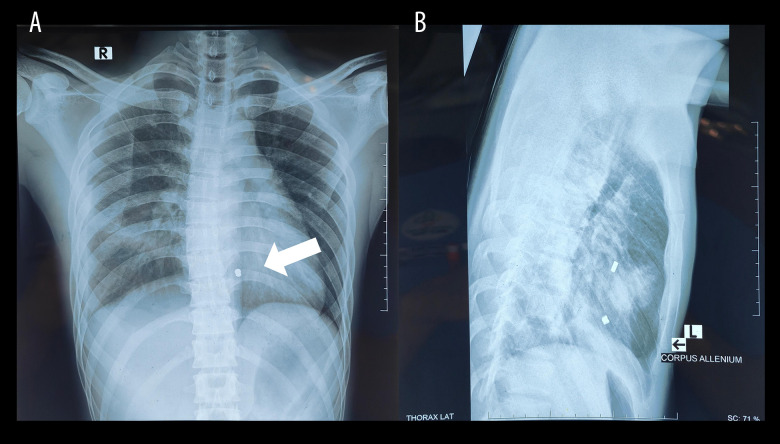
BACKGROUND Air rifles, frequently used in sports, can cause complex, violent, and traumatic cardiac injury associated with significant morbidity and mortality. Unlike firearm projectiles, air rifle pellets lack rotational movement but can achieve velocities of 100 to 230 m/s. CASE REPORT A 21-year-old man was referred to our hospital after sustaining an air rifle injury to the right chest. He presented 10 h after injury with chest pain but was hemodynamically stable. Physical examination revealed decreased breath sounds and tenderness in the right hemithorax. Chest X-ray showed right-sided hemothorax and pulmonary contusion, prompting chest tube placement, with initial drainage of 500 cc hemorrhagic fluid. Transthoracic echocardiography identified a hyperechoic mass in the right ventricle, with mild pericardial effusion. Computed tomography confirmed the projectile was lodged in the posterior right ventricle, 0.8 cm from the tricuspid annulus. Emergency surgery was performed and successfully extracted an intact 3×3×5 mm air gun pellet. Postoperatively, the patient experienced a brief tonic-clonic seizure, which was managed with midazolam and propofol. He received prophylactic ceftriaxone, intravenous phenytoin, vitamin B6, and folic acid and oral aspirin, ibuprofen, and omeprazole. The patient showed improvement by postoperative day 3 and was discharged on day 4. Weekly follow-ups and an EEG 1 month after discharge showed normal results. At the 2-month follow-up, the patient remained asymptomatic. CONCLUSIONS Awareness of cardiac penetrating wounds, bullet trajectory, and clinical signs, along with a multidisciplinary approach and patient-family involvement, is crucial for favorable outcomes and long-term follow-up.
期刊介绍:
American Journal of Case Reports is an international, peer-reviewed scientific journal that publishes single and series case reports in all medical fields. American Journal of Case Reports is issued on a continuous basis as a primary electronic journal. Print copies of a single article or a set of articles can be ordered on demand.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


