Assessment of Mental and Chronic Health Conditions as Determinants of Health Care Needs and Digital Innovations for Women With Sexual Dysfunction: Cross-Sectional Population-Based Survey Study in Germany.
Selina Marie Kronthaler, Tatjana Tissen-Diabaté, Maria Margarete Karsten, Jens-Uwe Blohmer, Klaus Michael Beier, Laura Hatzler
{"title":"Assessment of Mental and Chronic Health Conditions as Determinants of Health Care Needs and Digital Innovations for Women With Sexual Dysfunction: Cross-Sectional Population-Based Survey Study in Germany.","authors":"Selina Marie Kronthaler, Tatjana Tissen-Diabaté, Maria Margarete Karsten, Jens-Uwe Blohmer, Klaus Michael Beier, Laura Hatzler","doi":"10.2196/71301","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A chronic health condition (CHC) is a recognized risk factor for experiencing problems in sexual function (PSF). According to the International Classification of Diseases, 11th Revision (ICD-11), the development of severe symptoms of sexual distress is the defining criterion for clinically relevant sexual dysfunction. Data on the contribution of specific CHCs to clinically relevant sexual dysfunction symptoms and related health care needs are limited, hindering targeted interventions.</p><p><strong>Objective: </strong>This study examines the prevalence of PSF, sexual dysfunction, and sexual distress; assesses associations with CHC status; evaluates sexual dysfunction diagnoses; and explores health care preferences.</p><p><strong>Methods: </strong>Data collection in this cross-sectional population-based survey study was based on a questionnaire developed with patient and public involvement and administered by YouGov to a representative sample of adults in Germany. Analyses included 1970 women with and without CHCs and different CHC subgroups (mental health-related, gynecological, cardiovascular and metabolic, infectious and inflammatory, cancer, pain-related, and neurological). The outcomes measured were PSF, clinically relevant sexual dysfunction symptoms, sexual distress (Female Sexual Distress Scale-Desire/Arousal/Orgasm [FSDS-DAO]), and self-reported sexual dysfunction diagnoses. Multivariable regression and network analysis explored associations among CHC subgroups, PSF, sexual dysfunction, and FSDS-DAO scores.</p><p><strong>Results: </strong>Among 1970 cisgender women (mean age 49.6, SD 16.0 years), 1186 (60.2%) reported CHCs. The 6-month PSF prevalence was 75.2% (820/1090) in women with CHCs and 62.5% (399/638) in women without CHCs. Clinically relevant sexual dysfunction symptoms were less prevalent (CHC: 202/1046, 19.3% vs no CHC: 68/601, 11.3%). Multivariable regression models showed an association between sexual dysfunction and CHCs (odds ratio [OR] 2.56, 95% CI 1.90-3.49), which was the strongest for women with mental health-related CHCs (OR 2.31, 95% CI 1.70-3.13) and cancer CHCs (OR 2.00, 95% CI 1.45-2.78). Being in a relationship was a protective factor for clinically relevant distress among women with CHCs. Network analysis showed positive associations of PSF with gynecological and mental health-related CHCs and of sexual dysfunction with mental health-related, gynecological, and cancer CHCs. Women with sexual dysfunction symptoms reported low rates of sexual dysfunction diagnosis (CHC: 39/200, 19.4% vs no CHC: 6/55, 10.7%) and treatment (CHC: 16/146, 11.0% vs no CHC: 3/40, 7.0%). Gynecologists were the preferred health care providers for sexual dysfunction. The most commonly reported unmet need was a lack of information. Digital solutions, such as apps and websites with exercises, were desired as health care innovations.</p><p><strong>Conclusions: </strong>The burden of CHCs on women's sexual health extends beyond functional sexual impairment, with high rates of clinically relevant sexual distress. Cancer and mental health conditions are the strongest predictors of sexual dysfunction. Despite the high prevalence of sexual dysfunction in women with CHCs, access to diagnosis and treatment is limited. Digital offerings could help address these unmet needs.</p>","PeriodicalId":36208,"journal":{"name":"Journal of Participatory Medicine","volume":"17 ","pages":"e71301"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386550/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Participatory Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/71301","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A chronic health condition (CHC) is a recognized risk factor for experiencing problems in sexual function (PSF). According to the International Classification of Diseases, 11th Revision (ICD-11), the development of severe symptoms of sexual distress is the defining criterion for clinically relevant sexual dysfunction. Data on the contribution of specific CHCs to clinically relevant sexual dysfunction symptoms and related health care needs are limited, hindering targeted interventions.
Objective: This study examines the prevalence of PSF, sexual dysfunction, and sexual distress; assesses associations with CHC status; evaluates sexual dysfunction diagnoses; and explores health care preferences.
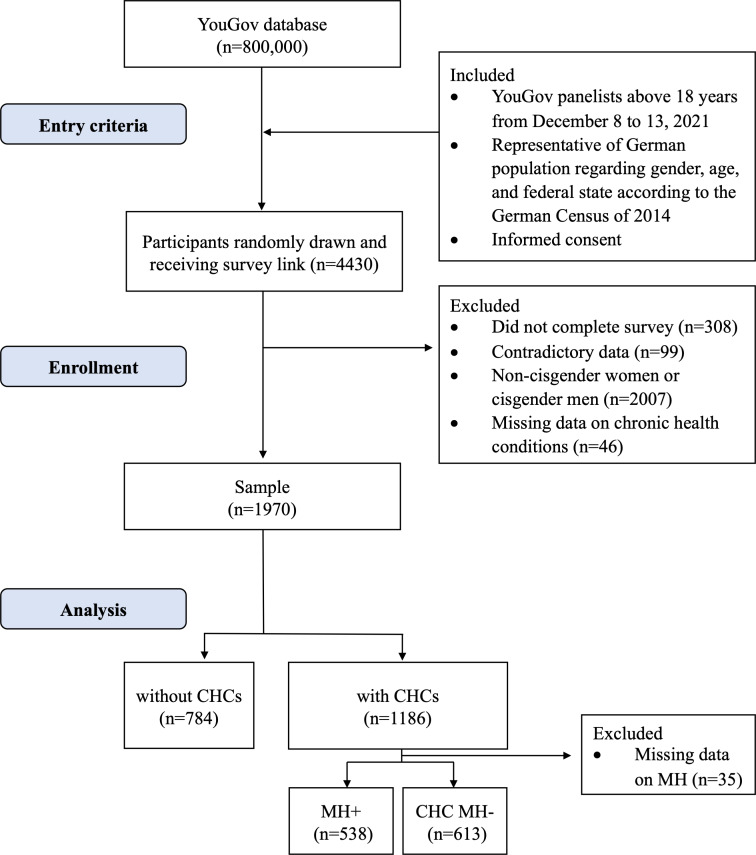
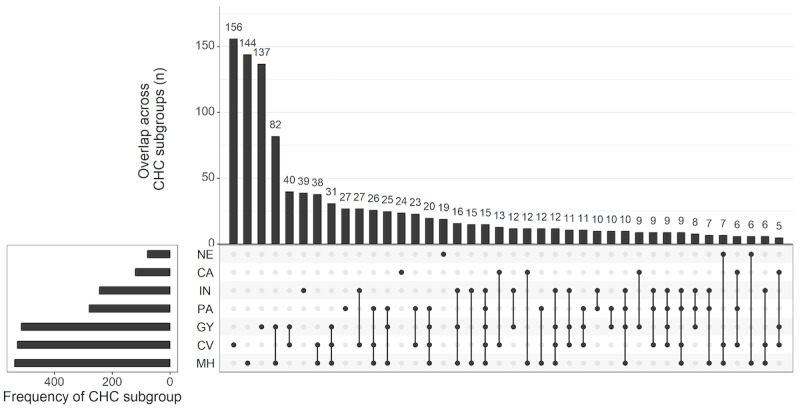
Methods: Data collection in this cross-sectional population-based survey study was based on a questionnaire developed with patient and public involvement and administered by YouGov to a representative sample of adults in Germany. Analyses included 1970 women with and without CHCs and different CHC subgroups (mental health-related, gynecological, cardiovascular and metabolic, infectious and inflammatory, cancer, pain-related, and neurological). The outcomes measured were PSF, clinically relevant sexual dysfunction symptoms, sexual distress (Female Sexual Distress Scale-Desire/Arousal/Orgasm [FSDS-DAO]), and self-reported sexual dysfunction diagnoses. Multivariable regression and network analysis explored associations among CHC subgroups, PSF, sexual dysfunction, and FSDS-DAO scores.
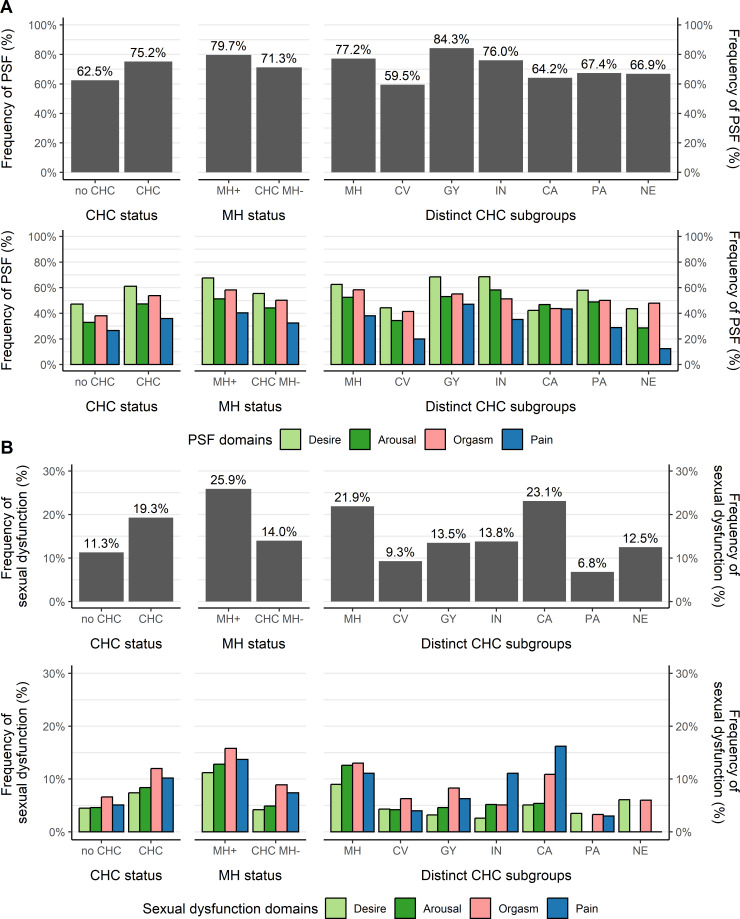
Results: Among 1970 cisgender women (mean age 49.6, SD 16.0 years), 1186 (60.2%) reported CHCs. The 6-month PSF prevalence was 75.2% (820/1090) in women with CHCs and 62.5% (399/638) in women without CHCs. Clinically relevant sexual dysfunction symptoms were less prevalent (CHC: 202/1046, 19.3% vs no CHC: 68/601, 11.3%). Multivariable regression models showed an association between sexual dysfunction and CHCs (odds ratio [OR] 2.56, 95% CI 1.90-3.49), which was the strongest for women with mental health-related CHCs (OR 2.31, 95% CI 1.70-3.13) and cancer CHCs (OR 2.00, 95% CI 1.45-2.78). Being in a relationship was a protective factor for clinically relevant distress among women with CHCs. Network analysis showed positive associations of PSF with gynecological and mental health-related CHCs and of sexual dysfunction with mental health-related, gynecological, and cancer CHCs. Women with sexual dysfunction symptoms reported low rates of sexual dysfunction diagnosis (CHC: 39/200, 19.4% vs no CHC: 6/55, 10.7%) and treatment (CHC: 16/146, 11.0% vs no CHC: 3/40, 7.0%). Gynecologists were the preferred health care providers for sexual dysfunction. The most commonly reported unmet need was a lack of information. Digital solutions, such as apps and websites with exercises, were desired as health care innovations.
Conclusions: The burden of CHCs on women's sexual health extends beyond functional sexual impairment, with high rates of clinically relevant sexual distress. Cancer and mental health conditions are the strongest predictors of sexual dysfunction. Despite the high prevalence of sexual dysfunction in women with CHCs, access to diagnosis and treatment is limited. Digital offerings could help address these unmet needs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


