{"title":"The Role of the Clinical Pharmacist in Hospital Admission Medication Reconciliation in Low-Resource Settings.","authors":"Tijana Kovačević, Sonja Nedinić, Vedrana Barišić, Branislava Miljković, Emir Fazlić, Slobodan Vukadinović, Pedja Kovačević","doi":"10.3390/pharmacy13040107","DOIUrl":null,"url":null,"abstract":"<p><p>Medication discrepancies at hospital admission are common and may lead to adverse outcomes. Medication reconciliation is a critical process for minimizing medication discrepancies and medication errors at the time of hospital admission. This study aimed to evaluate the role of clinical pharmacists in identifying pharmacotherapy-related issues upon patient admission in a low-resource setting. A prospective observational study was conducted at a university hospital between 1 March and 31 May 2023. Within 24 h of admission, a clinical pharmacist documented each patient's pre-admission medication regimen and compared it with the medication history obtained by the admitting physician. Discrepancies and pharmacotherapy problems were subsequently identified. Among 65 patients, pharmacists documented 334 medications versus 189 recorded by physicians (<i>p</i> < 0.01). The clinical pharmacist identified 155 discrepancies, 112 (72.26%) of which were unintentional. The most frequent type was drug omission (91.07%), followed by incorrect dosage (4.46%), incorrect dosing interval (2.68%), and medications with unknown indications (1.79%). Most discrepancies were classified as errors without harm (53.57%), while 41.07% were potentially harmful. These findings underscore the importance of integrating clinical pharmacists into the healthcare team. Their active participation during hospital admission can significantly enhance medication safety and reduce preventable adverse drug events.</p>","PeriodicalId":30544,"journal":{"name":"Pharmacy","volume":"13 4","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2025-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12388866/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pharmacy13040107","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
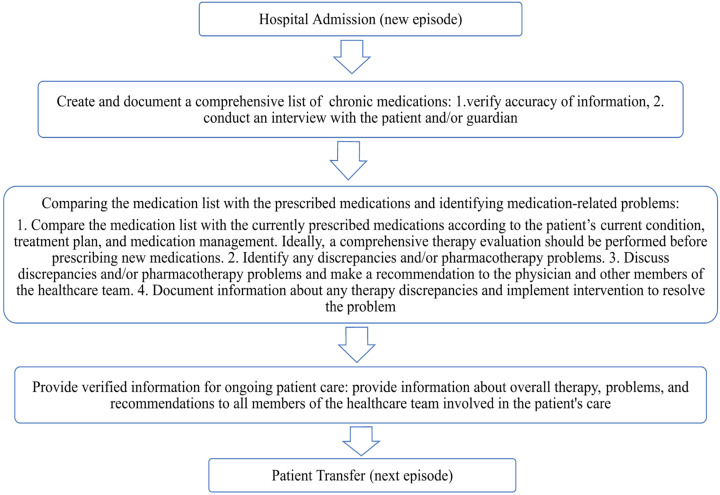
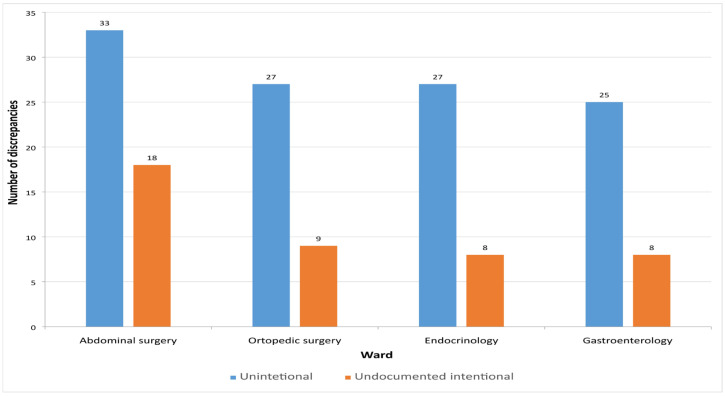
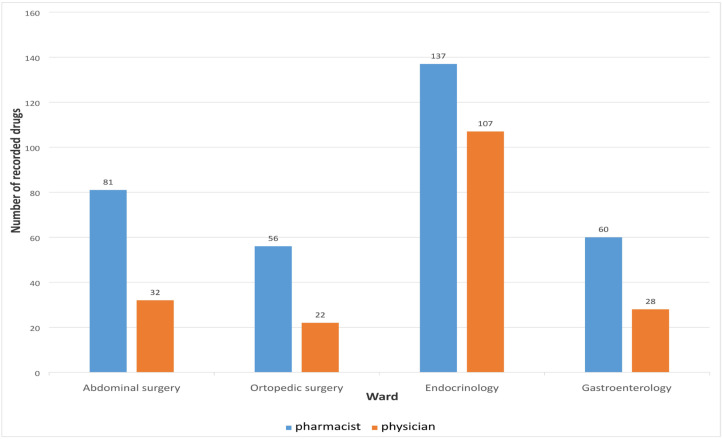
Medication discrepancies at hospital admission are common and may lead to adverse outcomes. Medication reconciliation is a critical process for minimizing medication discrepancies and medication errors at the time of hospital admission. This study aimed to evaluate the role of clinical pharmacists in identifying pharmacotherapy-related issues upon patient admission in a low-resource setting. A prospective observational study was conducted at a university hospital between 1 March and 31 May 2023. Within 24 h of admission, a clinical pharmacist documented each patient's pre-admission medication regimen and compared it with the medication history obtained by the admitting physician. Discrepancies and pharmacotherapy problems were subsequently identified. Among 65 patients, pharmacists documented 334 medications versus 189 recorded by physicians (p < 0.01). The clinical pharmacist identified 155 discrepancies, 112 (72.26%) of which were unintentional. The most frequent type was drug omission (91.07%), followed by incorrect dosage (4.46%), incorrect dosing interval (2.68%), and medications with unknown indications (1.79%). Most discrepancies were classified as errors without harm (53.57%), while 41.07% were potentially harmful. These findings underscore the importance of integrating clinical pharmacists into the healthcare team. Their active participation during hospital admission can significantly enhance medication safety and reduce preventable adverse drug events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


