Pharmacist-Led Interventions for Polypharmacy Management in Older Adults: A Systematic Review of Strategies and Outcomes in the United Kingdom and the Republic of Ireland.
{"title":"Pharmacist-Led Interventions for Polypharmacy Management in Older Adults: A Systematic Review of Strategies and Outcomes in the United Kingdom and the Republic of Ireland.","authors":"Fionnuala McGrory, Mohamed Hassan Elnaem","doi":"10.3390/pharmacy13040109","DOIUrl":null,"url":null,"abstract":"<p><p>Polypharmacy in older adults increases risks of adverse drug reactions (ADRs), hospitalisations, and mortality. Pharmacist-led interventions using validated tools (e.g., STOPP/START, MAI, STOPPFrail) aim to optimise prescribing, yet their impact on clinical and economic outcomes in UK/Ireland health systems remains underexplored. This systematic review aimed to critically assess the impact of pharmacist-led deprescribing interventions on PIP, clinical outcomes, and costs in older adults (≥65 years) across the UK and Ireland. Following PRISMA 2020 guidelines, four databases (PubMed, Scopus, Web of Science, Cochrane Library) were searched for studies (2010-2024). Eligible studies included randomised trials, observational designs, and intervention studies in hospitals, care homes, community pharmacies, and intermediate care settings. Fourteen studies met the inclusion criteria. The risk of bias was assessed using CASP checklists. Narrative syntheses and heat maps summarised the findings. Twelve of fourteen studies reported positive outcomes: reductions in potentially inappropriate medications, ADRs, medication burdens, and falls/fall risks. Medication appropriateness improved significantly in 35% of studies using the MAI. STOPPFrail reduced PIMs in care homes, while the MAI enhanced complex hospital reviews. Community interventions improved adherence and reduced the use of fall risk drugs. No studies demonstrated a reduction in hospitalisations, mortality, or the length of stays. Economic analyses showed mixed cost-effectiveness. Key barriers included low uptake of pharmacist recommendations and short follow-up periods. Pharmacist-led interventions have significantly improved the prescribing quality and reduced medication-related risks, but they fail to impact hospitalisations or mortality due to implementation gaps. Context-specific tools and policy reforms-including expanded pharmacist roles and electronic decision support-are critical for sustainability. Future research should focus on long-term outcomes, cost-effectiveness, and multidisciplinary integration.</p>","PeriodicalId":30544,"journal":{"name":"Pharmacy","volume":"13 4","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12389713/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pharmacy13040109","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
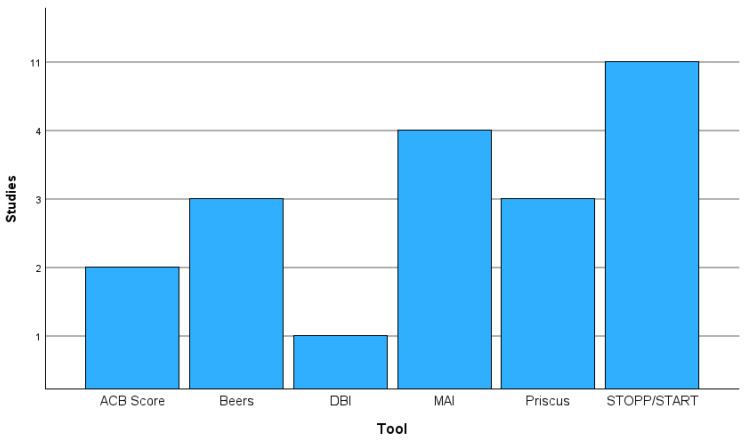
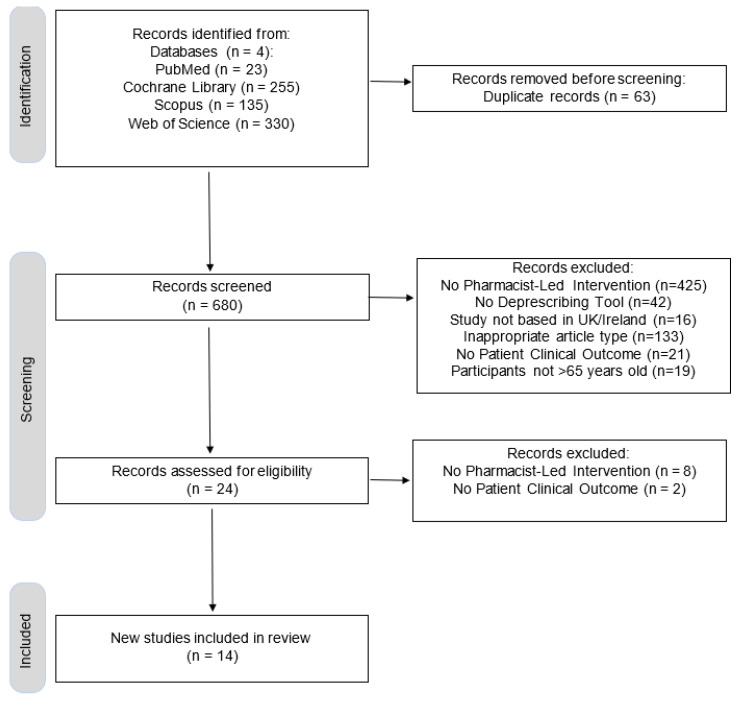
Polypharmacy in older adults increases risks of adverse drug reactions (ADRs), hospitalisations, and mortality. Pharmacist-led interventions using validated tools (e.g., STOPP/START, MAI, STOPPFrail) aim to optimise prescribing, yet their impact on clinical and economic outcomes in UK/Ireland health systems remains underexplored. This systematic review aimed to critically assess the impact of pharmacist-led deprescribing interventions on PIP, clinical outcomes, and costs in older adults (≥65 years) across the UK and Ireland. Following PRISMA 2020 guidelines, four databases (PubMed, Scopus, Web of Science, Cochrane Library) were searched for studies (2010-2024). Eligible studies included randomised trials, observational designs, and intervention studies in hospitals, care homes, community pharmacies, and intermediate care settings. Fourteen studies met the inclusion criteria. The risk of bias was assessed using CASP checklists. Narrative syntheses and heat maps summarised the findings. Twelve of fourteen studies reported positive outcomes: reductions in potentially inappropriate medications, ADRs, medication burdens, and falls/fall risks. Medication appropriateness improved significantly in 35% of studies using the MAI. STOPPFrail reduced PIMs in care homes, while the MAI enhanced complex hospital reviews. Community interventions improved adherence and reduced the use of fall risk drugs. No studies demonstrated a reduction in hospitalisations, mortality, or the length of stays. Economic analyses showed mixed cost-effectiveness. Key barriers included low uptake of pharmacist recommendations and short follow-up periods. Pharmacist-led interventions have significantly improved the prescribing quality and reduced medication-related risks, but they fail to impact hospitalisations or mortality due to implementation gaps. Context-specific tools and policy reforms-including expanded pharmacist roles and electronic decision support-are critical for sustainability. Future research should focus on long-term outcomes, cost-effectiveness, and multidisciplinary integration.
老年人使用多种药物会增加药物不良反应(adr)、住院和死亡率的风险。使用经过验证的工具(例如,STOPP/START, MAI, stopp虚弱)的药剂师主导的干预措施旨在优化处方,但其对英国/爱尔兰卫生系统的临床和经济结果的影响仍未得到充分探讨。本系统综述旨在批判性地评估药剂师主导的处方干预对英国和爱尔兰老年人(≥65岁)PIP、临床结果和成本的影响。按照PRISMA 2020指南,检索了四个数据库(PubMed, Scopus, Web of Science, Cochrane Library)的研究(2010-2024)。符合条件的研究包括在医院、护理院、社区药房和中间护理机构进行的随机试验、观察性设计和干预研究。14项研究符合纳入标准。使用CASP检查表评估偏倚风险。叙述性综合和热图总结了这些发现。14项研究中有12项报告了积极的结果:减少了潜在的不适当药物、不良反应、药物负担和跌倒/跌倒风险。在使用MAI的研究中,35%的用药适宜性显著改善。stopp虚弱减少了护理院的pim,而MAI增强了复杂的医院审查。社区干预提高了依从性并减少了跌倒风险药物的使用。没有研究表明住院率、死亡率或住院时间有所减少。经济分析显示成本效益好坏参半。主要障碍包括对药剂师建议的接受程度低和随访时间短。药剂师主导的干预措施大大提高了处方质量,降低了与药物有关的风险,但由于实施方面的差距,它们未能影响住院率或死亡率。针对具体情况的工具和政策改革——包括扩大药剂师角色和电子决策支持——对可持续性至关重要。未来的研究应关注长期结果、成本效益和多学科整合。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


