Trevor F Williams, James M Gold, James A Waltz, Jason Schiffman, Lauren M Ellman, Gregory P Strauss, Elaine F Walker, Scott W Woods, Albert R Powers, Joshua Kenney, Minerva K Pappu, Philip R Corlett, Tanya Tran, Steven M Silverstein, Richard E Zinbarg, Vijay A Mittal
{"title":"Identifying individuals at clinical high risk for psychosis using a battery of tasks sensitive to symptom mechanisms.","authors":"Trevor F Williams, James M Gold, James A Waltz, Jason Schiffman, Lauren M Ellman, Gregory P Strauss, Elaine F Walker, Scott W Woods, Albert R Powers, Joshua Kenney, Minerva K Pappu, Philip R Corlett, Tanya Tran, Steven M Silverstein, Richard E Zinbarg, Vijay A Mittal","doi":"10.1038/s41398-025-03539-5","DOIUrl":null,"url":null,"abstract":"<p><p>The clinical high risk for psychosis (CHR-P) population is important for understanding disease progression and treatment; however, standard approaches to identifying CHR-P individuals are expensive and labor-intensive. Focusing on neurocognitive mechanisms that underlie individual psychosis symptoms (positive, negative, and disorganization) may improve screening and identification. The present study examines whether a behavioral task battery that assays symptom mechanisms can identify CHR-P individuals and predict risk severity. Participants (N = 621) were recruited from clinics and the community as part of the Computerized Assessment of Psychosis Risk (CAPR) consortium study. Structured clinical interviews, a dimensional risk calculator, and behavioral tasks were administered. Clinical interviews identified the following groups: (a) CHR-P (n = 273), (b) non-CHR-P individuals with limited psychosis like experiences (PLEs; n = 120), (c) participants with mental disorders and no PLEs (CLN; n = 82), and (d) healthy controls (HC; n = 146). Multinomial logistic regression indicated that the task battery differentiated groups (p < 0.001), with utility for identifying CHR-P individuals (Sensitivity = 0.87, PPV = 0.51, NPV = 0.77), though with high false positives that varied based on comparison group (Specificity = 0.21-0.43). Tasks also predicted psychosis risk calculator scores (Adjusted R<sup>2</sup> = 0.12), with the two unique predictors being positive symptom task variables associated with updating beliefs regarding environmental volatility. Overall, symptom mechanism tasks differentiated CHR-P individuals from control groups, suggesting their potential as novel screening tools. Using tasks to more efficiently identify CHR-P individuals (e.g., enrich samples), may lower barriers and identify individuals that may otherwise be missed.</p>","PeriodicalId":23278,"journal":{"name":"Translational Psychiatry","volume":"15 1","pages":"311"},"PeriodicalIF":6.2000,"publicationDate":"2025-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12375010/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41398-025-03539-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
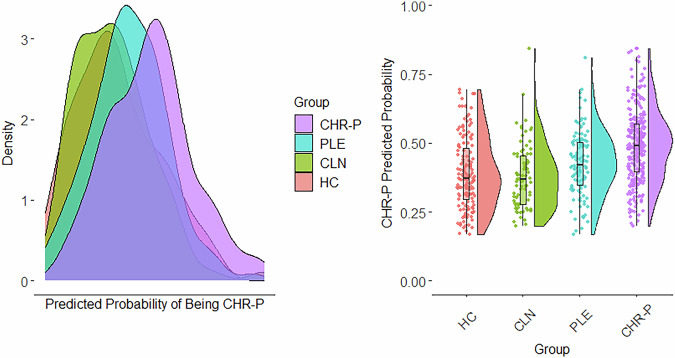
The clinical high risk for psychosis (CHR-P) population is important for understanding disease progression and treatment; however, standard approaches to identifying CHR-P individuals are expensive and labor-intensive. Focusing on neurocognitive mechanisms that underlie individual psychosis symptoms (positive, negative, and disorganization) may improve screening and identification. The present study examines whether a behavioral task battery that assays symptom mechanisms can identify CHR-P individuals and predict risk severity. Participants (N = 621) were recruited from clinics and the community as part of the Computerized Assessment of Psychosis Risk (CAPR) consortium study. Structured clinical interviews, a dimensional risk calculator, and behavioral tasks were administered. Clinical interviews identified the following groups: (a) CHR-P (n = 273), (b) non-CHR-P individuals with limited psychosis like experiences (PLEs; n = 120), (c) participants with mental disorders and no PLEs (CLN; n = 82), and (d) healthy controls (HC; n = 146). Multinomial logistic regression indicated that the task battery differentiated groups (p < 0.001), with utility for identifying CHR-P individuals (Sensitivity = 0.87, PPV = 0.51, NPV = 0.77), though with high false positives that varied based on comparison group (Specificity = 0.21-0.43). Tasks also predicted psychosis risk calculator scores (Adjusted R2 = 0.12), with the two unique predictors being positive symptom task variables associated with updating beliefs regarding environmental volatility. Overall, symptom mechanism tasks differentiated CHR-P individuals from control groups, suggesting their potential as novel screening tools. Using tasks to more efficiently identify CHR-P individuals (e.g., enrich samples), may lower barriers and identify individuals that may otherwise be missed.
期刊介绍:
Psychiatry has suffered tremendously by the limited translational pipeline. Nobel laureate Julius Axelrod''s discovery in 1961 of monoamine reuptake by pre-synaptic neurons still forms the basis of contemporary antidepressant treatment. There is a grievous gap between the explosion of knowledge in neuroscience and conceptually novel treatments for our patients. Translational Psychiatry bridges this gap by fostering and highlighting the pathway from discovery to clinical applications, healthcare and global health. We view translation broadly as the full spectrum of work that marks the pathway from discovery to global health, inclusive. The steps of translation that are within the scope of Translational Psychiatry include (i) fundamental discovery, (ii) bench to bedside, (iii) bedside to clinical applications (clinical trials), (iv) translation to policy and health care guidelines, (v) assessment of health policy and usage, and (vi) global health. All areas of medical research, including — but not restricted to — molecular biology, genetics, pharmacology, imaging and epidemiology are welcome as they contribute to enhance the field of translational psychiatry.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


