Aikaterini Anastasiou, Alex Brehm, Johannes Kaesmacher, Adnan Mujanovic, Marta de Dios Lascuevas, Tomás Carmona Fuentes, Alfonso López-Frías, Blanca Hidalgo Valverde, Ansgar Berlis, Christoph J Maurer, Thanh N Nguyen, Mohamad Abdalkader, Piers Klein, Guillaume Thevoz, Patrik Michel, Bruno Bartolini, Marius Kaschner, Daniel Weiss, Andrea M Alexandre, Alessandro Pedicelli, Paolo Machi, Gianmarco Bernava, Shuntaro Kuwahara, Kazutaka Uchida, Jason Wenderoth, Anirudh Joshi, Grzegorz Karwacki, Manuel Bolognese, Agostino Tessitore, Sergio Lucio Vinci, Amedeo Cervo, Claudia Rollo, Ferdinand Hui, Aaisha Siddiqua Mozumder, Daniele Giuseppe Romano, Giulia Frauenfelder, Nitin Goyal, Vivek Batra, Violiza Inoa, Christophe Cognard, Matúš Hoferica, Riitta Rautio, Daniel P O Kaiser, Johannes C Gerber, Julian Clarke, Michael R Levitt, Marcel N Wolf, Ahmed E Othman, Luca Scarcia, Erwah Kalsoum, Diana Melancia, Diana Aguiar de Sousa, Maria Porzia Ganimede, Vittorio Semeraro, Flavio Giordano, Massimo Muto, Aristeidis Katsanos, Umesh Bonala, Anil M Tuladhar, Sjoerd F M Jenniskens, Victoria Hellstern, Ilka Kleffner, Paolo Remida, Susanna Diamanti, Leonardo Renieri, Elena Ballabio, Luca Valvassori, Nikki Rommers, Mira Katan, Victor Schulze-Zachau, Marios-Nikos Psychogios
{"title":"Platelet inhibition strategies in rescue stenting after failed thrombectomy: a large retrospective multicenter registry.","authors":"Aikaterini Anastasiou, Alex Brehm, Johannes Kaesmacher, Adnan Mujanovic, Marta de Dios Lascuevas, Tomás Carmona Fuentes, Alfonso López-Frías, Blanca Hidalgo Valverde, Ansgar Berlis, Christoph J Maurer, Thanh N Nguyen, Mohamad Abdalkader, Piers Klein, Guillaume Thevoz, Patrik Michel, Bruno Bartolini, Marius Kaschner, Daniel Weiss, Andrea M Alexandre, Alessandro Pedicelli, Paolo Machi, Gianmarco Bernava, Shuntaro Kuwahara, Kazutaka Uchida, Jason Wenderoth, Anirudh Joshi, Grzegorz Karwacki, Manuel Bolognese, Agostino Tessitore, Sergio Lucio Vinci, Amedeo Cervo, Claudia Rollo, Ferdinand Hui, Aaisha Siddiqua Mozumder, Daniele Giuseppe Romano, Giulia Frauenfelder, Nitin Goyal, Vivek Batra, Violiza Inoa, Christophe Cognard, Matúš Hoferica, Riitta Rautio, Daniel P O Kaiser, Johannes C Gerber, Julian Clarke, Michael R Levitt, Marcel N Wolf, Ahmed E Othman, Luca Scarcia, Erwah Kalsoum, Diana Melancia, Diana Aguiar de Sousa, Maria Porzia Ganimede, Vittorio Semeraro, Flavio Giordano, Massimo Muto, Aristeidis Katsanos, Umesh Bonala, Anil M Tuladhar, Sjoerd F M Jenniskens, Victoria Hellstern, Ilka Kleffner, Paolo Remida, Susanna Diamanti, Leonardo Renieri, Elena Ballabio, Luca Valvassori, Nikki Rommers, Mira Katan, Victor Schulze-Zachau, Marios-Nikos Psychogios","doi":"10.1177/17562864251360913","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rescue stenting (RS) is a bailout strategy for failed thrombectomy. Optimal platelet inhibition strategy after RS remains unclear.</p><p><strong>Objectives: </strong>We aimed to describe and compare different platelet inhibition strategies during/after RS.</p><p><strong>Design: </strong>Retrospective cohort study across 34 international centers.</p><p><strong>Methods: </strong>Patients with large vessel occlusion and RS after failed thrombectomy (2019-2023) were included. Periprocedural and postprocedural platelet inhibition strategies were described and compared, focusing on glycoprotein IIb/IIIa (GPIIb/IIIa) inhibitors, single antiplatelet therapy (SAPT), and dual antiplatelet therapy (DAPT). We assessed the effects of platelet inhibition strategy and potentially covariates on the primary outcome of 90-day modified Rankin Scale (mRS) using ordinal shift analysis with proportional odds models.</p><p><strong>Results: </strong>RS was performed in 589 patients (mean age 67.9 years, 60.8% male). Numerous combinations of platelet inhibitors were administered. Periprocedural GPIIb/IIIa inhibitors were used in 61.5% of patients. Postprocedural DAPT was administered to 80.5% and SAPT to 13.3%. Functional independence (mRS 0-2) was achieved in 40.7%, while 26.3% died within 90 days. Stent occlusion occurred in 20.5%, with 67.6% of these occlusions within 24 h. Postprocedural stent-occlusion was independently associated with worse functional outcome at 90 days (OR 4.1, 95% CI 2.3-7.2, <i>p</i> < 0.001). No significant association between periprocedural GPIIb/IIIa inhibitors, and 90-day mRS or stent occlusion was found. Postprocedural SAPT was associated with worse functional outcomes (adjusted odds ratio (aOR) 2.4, 95% CI 1.1-5.0, <i>p</i> = 0.02), higher mortality (aOR 2.1, 95% CI 1.05-4.0, <i>p</i> = 0.03), and increased stent occlusion rates (aOR 4.8, 95% CI 2.3-9.7, <i>p</i> < 0.001) compared to postprocedural DAPT. Symptomatic intracranial hemorrhage occurred in 6.8% of patients, with no significant difference between antiplatelet regimens.</p><p><strong>Conclusion: </strong>Extensive heterogeneity exists in platelet inhibition strategies following RS. Stent occlusion is associated with worse clinical outcomes, and the first 24 h post-RS are critical for stent patency. Compared to SAPT, DAPT was associated with better functional outcome, lower mortality, and lower stent occlusion rates.</p>","PeriodicalId":22980,"journal":{"name":"Therapeutic Advances in Neurological Disorders","volume":"18 ","pages":"17562864251360913"},"PeriodicalIF":4.1000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374045/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Neurological Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562864251360913","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Rescue stenting (RS) is a bailout strategy for failed thrombectomy. Optimal platelet inhibition strategy after RS remains unclear.
Objectives: We aimed to describe and compare different platelet inhibition strategies during/after RS.
Design: Retrospective cohort study across 34 international centers.
Methods: Patients with large vessel occlusion and RS after failed thrombectomy (2019-2023) were included. Periprocedural and postprocedural platelet inhibition strategies were described and compared, focusing on glycoprotein IIb/IIIa (GPIIb/IIIa) inhibitors, single antiplatelet therapy (SAPT), and dual antiplatelet therapy (DAPT). We assessed the effects of platelet inhibition strategy and potentially covariates on the primary outcome of 90-day modified Rankin Scale (mRS) using ordinal shift analysis with proportional odds models.
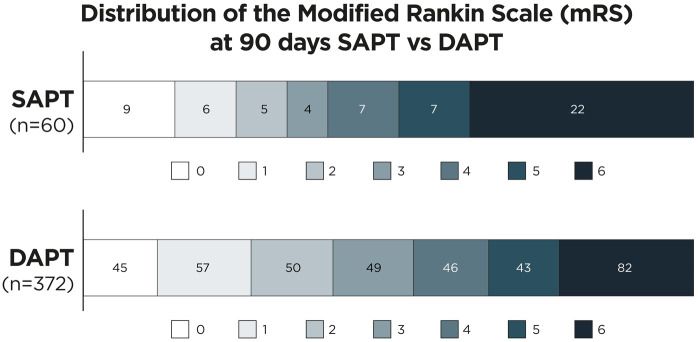
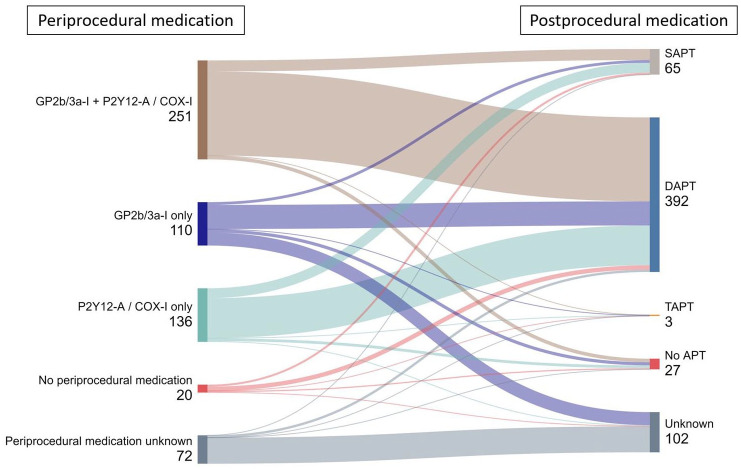
Results: RS was performed in 589 patients (mean age 67.9 years, 60.8% male). Numerous combinations of platelet inhibitors were administered. Periprocedural GPIIb/IIIa inhibitors were used in 61.5% of patients. Postprocedural DAPT was administered to 80.5% and SAPT to 13.3%. Functional independence (mRS 0-2) was achieved in 40.7%, while 26.3% died within 90 days. Stent occlusion occurred in 20.5%, with 67.6% of these occlusions within 24 h. Postprocedural stent-occlusion was independently associated with worse functional outcome at 90 days (OR 4.1, 95% CI 2.3-7.2, p < 0.001). No significant association between periprocedural GPIIb/IIIa inhibitors, and 90-day mRS or stent occlusion was found. Postprocedural SAPT was associated with worse functional outcomes (adjusted odds ratio (aOR) 2.4, 95% CI 1.1-5.0, p = 0.02), higher mortality (aOR 2.1, 95% CI 1.05-4.0, p = 0.03), and increased stent occlusion rates (aOR 4.8, 95% CI 2.3-9.7, p < 0.001) compared to postprocedural DAPT. Symptomatic intracranial hemorrhage occurred in 6.8% of patients, with no significant difference between antiplatelet regimens.
Conclusion: Extensive heterogeneity exists in platelet inhibition strategies following RS. Stent occlusion is associated with worse clinical outcomes, and the first 24 h post-RS are critical for stent patency. Compared to SAPT, DAPT was associated with better functional outcome, lower mortality, and lower stent occlusion rates.
背景:抢救支架置入术(RS)是对血栓切除失败的救助策略。RS后的最佳血小板抑制策略尚不清楚。目的:我们旨在描述和比较rs期间/之后不同的血小板抑制策略。设计:34个国际中心的回顾性队列研究。方法:纳入2019-2023年大血管闭塞合并取栓失败RS患者。对术中和术后血小板抑制策略进行了描述和比较,重点是糖蛋白IIb/IIIa (GPIIb/IIIa)抑制剂、单一抗血小板治疗(SAPT)和双重抗血小板治疗(DAPT)。我们使用比例优势模型的序移分析评估了血小板抑制策略和潜在协变量对90天修正兰金量表(mRS)主要结局的影响。结果:589例患者行RS,平均年龄67.9岁,男性60.8%。给予多种血小板抑制剂组合。61.5%的患者在手术期间使用了GPIIb/IIIa抑制剂。术后DAPT占80.5%,SAPT占13.3%。功能独立(mRS 0-2)达到40.7%,90天内死亡26.3%。20.5%发生支架闭塞,其中67.6%发生在24小时内。术后支架闭塞与术后90天较差的功能结果(OR 4.1, 95% CI 2.3-7.2, p p = 0.02)、较高的死亡率(aOR 2.1, 95% CI 1.05-4.0, p = 0.03)和支架闭塞率增加(aOR 4.8, 95% CI 2.3-9.7, p)独立相关。结论:RS后血小板抑制策略存在广泛的异质性。支架闭塞与较差的临床结果相关,RS后的前24小时是支架通畅的关键。与SAPT相比,DAPT具有更好的功能结局、更低的死亡率和更低的支架闭塞率。
期刊介绍:
Therapeutic Advances in Neurological Disorders is a peer-reviewed, open access journal delivering the highest quality articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of neurology. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in neurology, providing a forum in print and online for publishing the highest quality articles in this area.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


