Impact of Paravertebral Muscle Degeneration on Residual Low Back Pain Following Percutaneous Kyphoplasty for Osteoporotic Vertebral Fractures: A Retrospective Study.
Tao Feng, Shengyang Jin, Junjie Niu, Qi Yan, Dawei Song, Jinning Wang
{"title":"Impact of Paravertebral Muscle Degeneration on Residual Low Back Pain Following Percutaneous Kyphoplasty for Osteoporotic Vertebral Fractures: A Retrospective Study.","authors":"Tao Feng, Shengyang Jin, Junjie Niu, Qi Yan, Dawei Song, Jinning Wang","doi":"10.2147/PROM.S529923","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Residual low back pain (LBP) is frequently reported after percutaneous kyphoplasty (PKP) for osteoporotic vertebral fractures (OVFs), yet its underlying mechanisms remain unclear. Paravertebral muscles (PVMs) degeneration, particularly fat infiltration and atrophy may contribute to persistent postoperative pain.</p><p><strong>Objective: </strong>To evaluate the association between PVMs degeneration and residual LBP after PKP and identify imaging-based predictors for risk stratification.</p><p><strong>Methods: </strong>This retrospective cohort study included 213 patients (mean age 70.88 ± 8.58 years; 82.2% female) with single-level OVFs who underwent PKP between January 2021 and June 2023. Patients with multiple-level fractures, chronic LBP, neurological deficits, prior spinal surgery, incomplete imaging, or inadequate follow-up were excluded. Fat infiltration percentage (FI%) and cross-sectional area of the multifidus (MF), erector spinae (ES), and psoas major (PS) were measured at the L4 level using transverse T2-weighted MRI. Residual LBP was defined as postoperative VAS ≥3.5 at 12-month follow-up. Logistic regression and ROC analyses were conducted and appropriate univariate tests (<i>t</i>-test or Mann-Whitney <i>U</i>-test) were performed.</p><p><strong>Results: </strong>Residual LBP occurred in 13.6% of patients and was associated with higher VBQ scores (3.14 ± 0.38 vs 2.57 ± 0.25, P=0.001), greater postoperative kyphosis (16.03 ± 6.69° vs 6.70 ± 4.80°, <i>P</i>=0.001), increased FI% of ES/MF (57.28 ± 5.63% vs 43.40 ± 14.93%, <i>P</i>=0.001), reduced PS area (10.74 ± 4.23 cm² vs 16.15 ± 3.71 cm², <i>P</i>=0.001), and concentrated cement distribution (11.5% vs 73.6%, P=0.001). Independent predictors included elevated VBQ (OR=85.2, 95% CI 7.006-1036.458), kyphosis (OR=1.14, 95% CI 1.017-1.276), FI% of ES/MF (OR=1.082, 95% CI 1.008-1.160), and PS area (OR=0.509, 95% CI 0.285-0.910). ROC analysis identified FI% ≥49.78% and PS area ≤11.937 cm² as optimal cutoffs.</p><p><strong>Conclusion: </strong>Preoperative magnetic resonance imaging assessment of paravertebral muscle may help identify patients at risk for residual low back pain after kyphoplasty. Incorporating preoperative imaging and postoperative physical therapy referral may improve patient outcomes.</p>","PeriodicalId":19747,"journal":{"name":"Patient Related Outcome Measures","volume":"16 ","pages":"117-127"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12368434/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Related Outcome Measures","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/PROM.S529923","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Residual low back pain (LBP) is frequently reported after percutaneous kyphoplasty (PKP) for osteoporotic vertebral fractures (OVFs), yet its underlying mechanisms remain unclear. Paravertebral muscles (PVMs) degeneration, particularly fat infiltration and atrophy may contribute to persistent postoperative pain.
Objective: To evaluate the association between PVMs degeneration and residual LBP after PKP and identify imaging-based predictors for risk stratification.
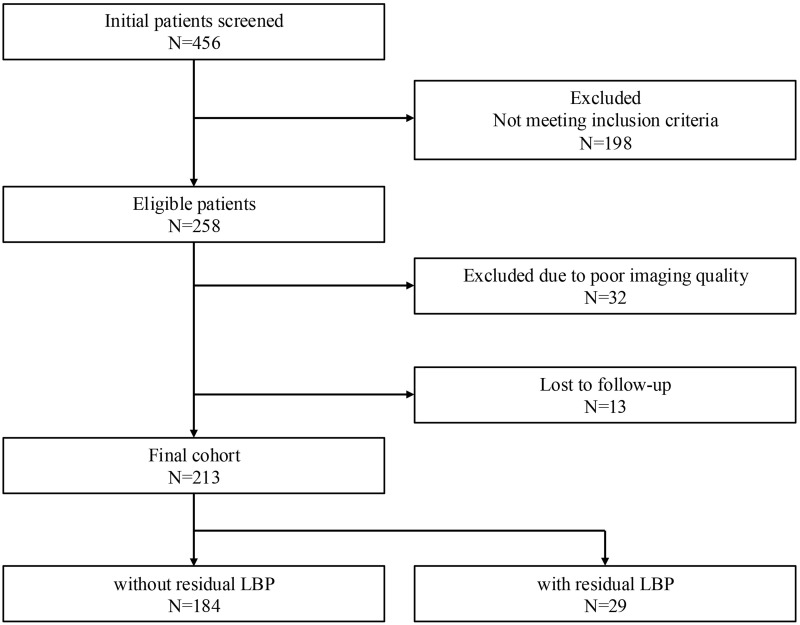
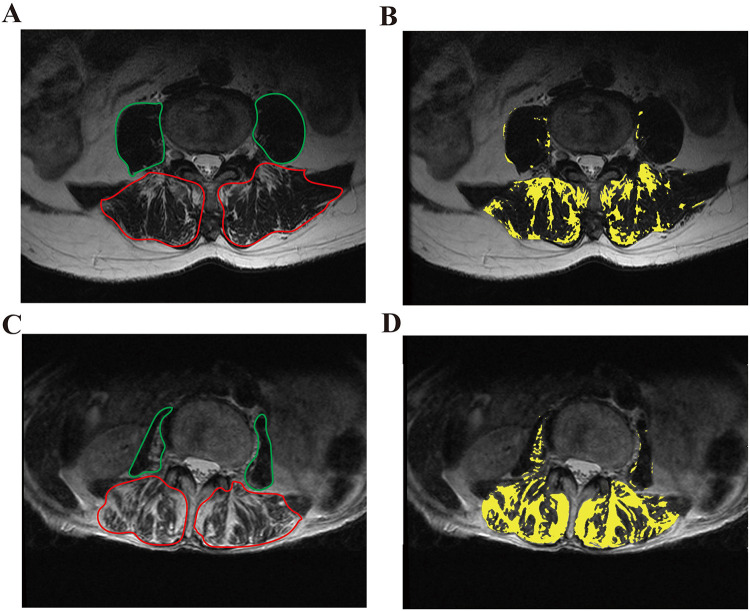
Methods: This retrospective cohort study included 213 patients (mean age 70.88 ± 8.58 years; 82.2% female) with single-level OVFs who underwent PKP between January 2021 and June 2023. Patients with multiple-level fractures, chronic LBP, neurological deficits, prior spinal surgery, incomplete imaging, or inadequate follow-up were excluded. Fat infiltration percentage (FI%) and cross-sectional area of the multifidus (MF), erector spinae (ES), and psoas major (PS) were measured at the L4 level using transverse T2-weighted MRI. Residual LBP was defined as postoperative VAS ≥3.5 at 12-month follow-up. Logistic regression and ROC analyses were conducted and appropriate univariate tests (t-test or Mann-Whitney U-test) were performed.
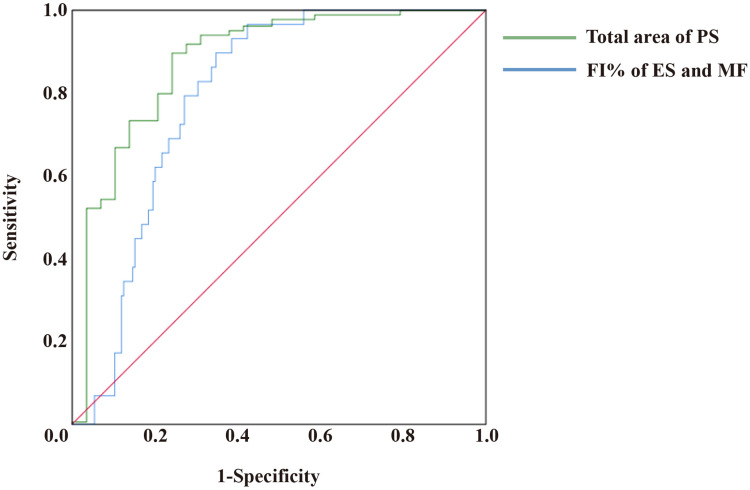
Results: Residual LBP occurred in 13.6% of patients and was associated with higher VBQ scores (3.14 ± 0.38 vs 2.57 ± 0.25, P=0.001), greater postoperative kyphosis (16.03 ± 6.69° vs 6.70 ± 4.80°, P=0.001), increased FI% of ES/MF (57.28 ± 5.63% vs 43.40 ± 14.93%, P=0.001), reduced PS area (10.74 ± 4.23 cm² vs 16.15 ± 3.71 cm², P=0.001), and concentrated cement distribution (11.5% vs 73.6%, P=0.001). Independent predictors included elevated VBQ (OR=85.2, 95% CI 7.006-1036.458), kyphosis (OR=1.14, 95% CI 1.017-1.276), FI% of ES/MF (OR=1.082, 95% CI 1.008-1.160), and PS area (OR=0.509, 95% CI 0.285-0.910). ROC analysis identified FI% ≥49.78% and PS area ≤11.937 cm² as optimal cutoffs.
Conclusion: Preoperative magnetic resonance imaging assessment of paravertebral muscle may help identify patients at risk for residual low back pain after kyphoplasty. Incorporating preoperative imaging and postoperative physical therapy referral may improve patient outcomes.
背景:骨质疏松性椎体骨折(ovf)经皮后凸成形术(PKP)后残留腰痛(LBP)经常被报道,但其潜在机制尚不清楚。椎旁肌肉(pvm)变性,特别是脂肪浸润和萎缩可能导致术后持续疼痛。目的:评估pvm退变与PKP后残留LBP之间的关系,并确定基于影像学的风险分层预测因素。方法:该回顾性队列研究包括213例在2021年1月至2023年6月期间接受PKP治疗的单级ovf患者(平均年龄70.88±8.58岁,82.2%为女性)。排除多节段骨折、慢性腰痛、神经功能缺损、既往脊柱手术、影像不完整或随访不充分的患者。采用横t2加权MRI在L4水平测量多裂肌(MF)、竖脊肌(ES)和大腰肌(PS)的脂肪浸润率(FI%)和横截面积。12个月随访时,残馀腰痛定义为术后VAS≥3.5。进行Logistic回归和ROC分析,并进行适当的单因素检验(t检验或Mann-Whitney u检验)。结果:13.6%的患者存在腰痛残留,与较高的VBQ评分(3.14±0.38 vs 2.57±0.25,P=0.001)、较大的术后后凸(16.03±6.69°vs 6.70±4.80°,P=0.001)、ES/MF的FI%增加(57.28±5.63% vs 43.40±14.93%,P=0.001)、PS面积减少(10.74±4.23 cm²vs 16.15±3.71 cm²,P=0.001)、水泥分布集中(11.5% vs 73.6%, P=0.001)相关。独立预测因子包括VBQ升高(OR=85.2, 95% CI 7.006-1036.458)、后凸(OR=1.14, 95% CI 1.017-1.276)、ES/MF的FI% (OR=1.082, 95% CI 1.008-1.160)和PS面积(OR=0.509, 95% CI 0.280 -0.910)。ROC分析确定FI%≥49.78%和PS面积≤11.937 cm²为最佳截止点。结论:椎旁肌肉的术前磁共振成像评估有助于识别后凸成形术后存在腰痛残留风险的患者。结合术前影像学和术后物理治疗转诊可改善患者预后。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


