{"title":"Sex Differences in Clinical Outcomes and Surgical Interventions for Infective Endocarditis: A Nationwide Registry.","authors":"Ching-Yi Lin, Feng-Cheng Chang, Chun-Yu Chen, Yu-Ting Cheng, Chia-Pin Lin, Ming-Jer Hsieh, Yi-Hsin Chan, Victor Chien-Chia Wu, An-Hsun Chou, Shao-Wei Chen","doi":"10.1093/ofid/ofaf473","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sex differences in infective endocarditis (IE) remain underexplored in large-scale studies. Current findings on clinical outcomes, particularly in surgical IE, are inconsistent, highlighting critical knowledge gaps.</p><p><strong>Methods: </strong>We conducted a nationwide cohort study using the Taiwan National Health Insurance Research Database (2001-2022) and a total of 28 976 adults with IE were identified. Subgroup analysis focused on 4133 patients undergoing valve surgery. Primary outcomes included in-hospital mortality and long-term survival, analyzed using logistic regression and Cox models.</p><p><strong>Results: </strong>Of 28 976 patients, 4133 underwent surgery (women/men: 10 580/18 396 overall; 1252/2881 surgical). Women were older with more comorbidities. After propensity score matching, women had higher in-hospital mortality in both the general cohort (21.2% vs 19.8%; odds ratio [OR]: 1.09, 95% confidence interval [CI]: 1.02-1.17) and surgical subgroup (20.7% vs 13.3%; OR: 1.70, 95% CI: 1.37-2.11). Women undergoing surgery had more perioperative complications, including postcardiotomy cardiogenic shock (10.5% vs 7.8%) and de novo dialysis (13.5% vs 9.8%). Long-term mortality was lower in women, while women in the surgical subgroup had higher mortality (hazard ratio [HR]: 1.12, 95% CI: 1.01-1.25) and redo valve surgery rates (11.5% vs 8.1%; HR: 1.43; 95% CI: 1.07-1.90).</p><p><strong>Conclusions: </strong>Women with IE had higher in-hospital mortality regardless of surgical intervention. Among those who underwent surgery, women experienced more perioperative complications compared with men. Although women exhibited superior overall late survival, those undergoing surgery had worse long-term outcomes. These findings highlight the need for improved sex-specific management, including early diagnosis, timely surgery, and extended follow-up.</p>","PeriodicalId":19517,"journal":{"name":"Open Forum Infectious Diseases","volume":"12 8","pages":"ofaf473"},"PeriodicalIF":3.8000,"publicationDate":"2025-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372668/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Forum Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ofid/ofaf473","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sex differences in infective endocarditis (IE) remain underexplored in large-scale studies. Current findings on clinical outcomes, particularly in surgical IE, are inconsistent, highlighting critical knowledge gaps.
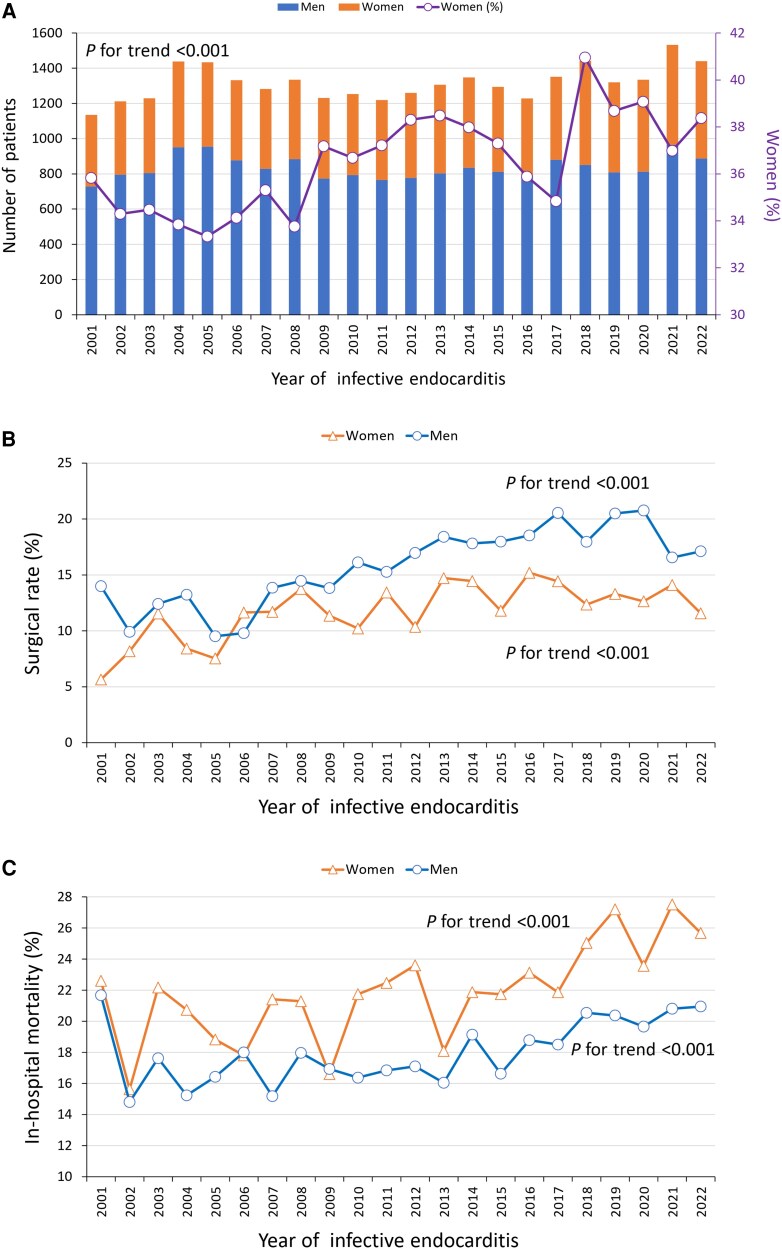
Methods: We conducted a nationwide cohort study using the Taiwan National Health Insurance Research Database (2001-2022) and a total of 28 976 adults with IE were identified. Subgroup analysis focused on 4133 patients undergoing valve surgery. Primary outcomes included in-hospital mortality and long-term survival, analyzed using logistic regression and Cox models.
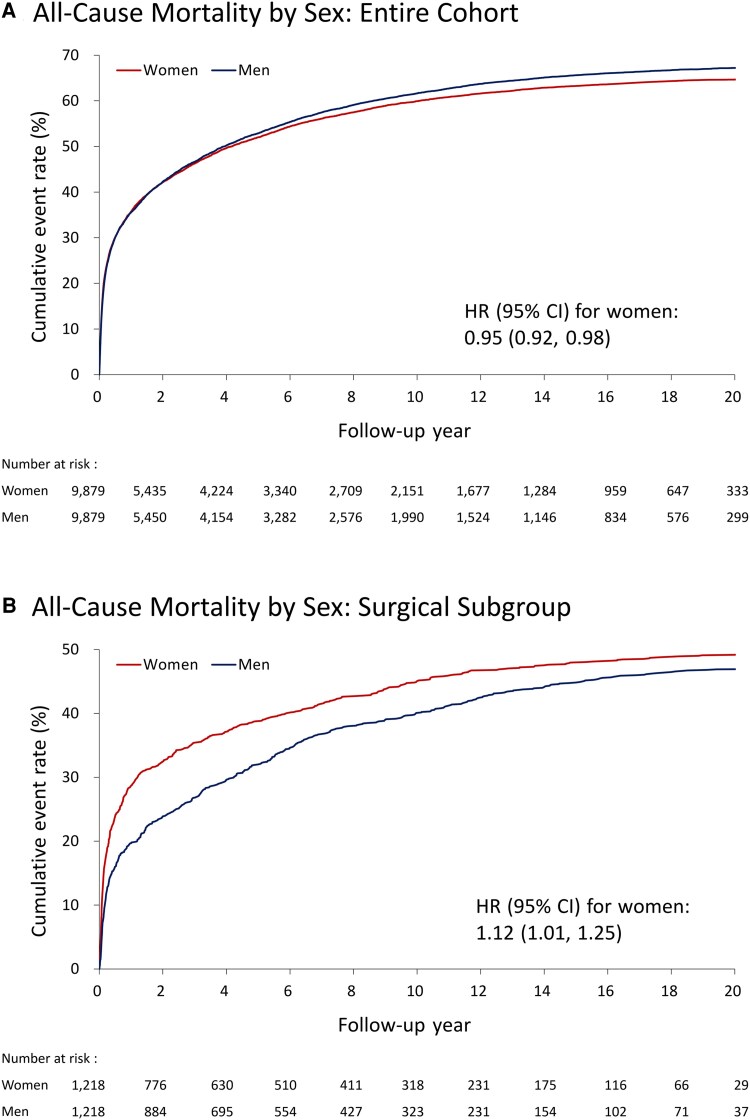
Results: Of 28 976 patients, 4133 underwent surgery (women/men: 10 580/18 396 overall; 1252/2881 surgical). Women were older with more comorbidities. After propensity score matching, women had higher in-hospital mortality in both the general cohort (21.2% vs 19.8%; odds ratio [OR]: 1.09, 95% confidence interval [CI]: 1.02-1.17) and surgical subgroup (20.7% vs 13.3%; OR: 1.70, 95% CI: 1.37-2.11). Women undergoing surgery had more perioperative complications, including postcardiotomy cardiogenic shock (10.5% vs 7.8%) and de novo dialysis (13.5% vs 9.8%). Long-term mortality was lower in women, while women in the surgical subgroup had higher mortality (hazard ratio [HR]: 1.12, 95% CI: 1.01-1.25) and redo valve surgery rates (11.5% vs 8.1%; HR: 1.43; 95% CI: 1.07-1.90).
Conclusions: Women with IE had higher in-hospital mortality regardless of surgical intervention. Among those who underwent surgery, women experienced more perioperative complications compared with men. Although women exhibited superior overall late survival, those undergoing surgery had worse long-term outcomes. These findings highlight the need for improved sex-specific management, including early diagnosis, timely surgery, and extended follow-up.
期刊介绍:
Open Forum Infectious Diseases provides a global forum for the publication of clinical, translational, and basic research findings in a fully open access, online journal environment. The journal reflects the broad diversity of the field of infectious diseases, and focuses on the intersection of biomedical science and clinical practice, with a particular emphasis on knowledge that holds the potential to improve patient care in populations around the world. Fully peer-reviewed, OFID supports the international community of infectious diseases experts by providing a venue for articles that further the understanding of all aspects of infectious diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


