Jasper Koolwijk, Mileen van de Kar, Brittney A van der Woude, Marcel van 't Veer, Harm Jan de Grooth, Harry J G M Crijns, Lukas R C Dekker, R Arthur Bouwman, Olaf L Cremer, Ashley J R de Bie, Luuk C Otterspoor
{"title":"Anticoagulation and thromboembolic risk in critically ill patients with trigger-induced atrial fibrillation-A systematic review and meta-analysis.","authors":"Jasper Koolwijk, Mileen van de Kar, Brittney A van der Woude, Marcel van 't Veer, Harm Jan de Grooth, Harry J G M Crijns, Lukas R C Dekker, R Arthur Bouwman, Olaf L Cremer, Ashley J R de Bie, Luuk C Otterspoor","doi":"10.1007/s12471-025-01978-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In critically ill patients with trigger-induced atrial fibrillation, there are no definitive recommendations on the use of anticoagulation. This study aimed to evaluate the association between anticoagulation therapy and outcomes (i.e. thromboembolism, bleeding and mortality) and examine prescription patterns in high-risk individuals based on CHA<sub>2</sub>DS<sub>2</sub>-VASc scores.</p><p><strong>Methods: </strong>A systematic search was conducted to identify studies reporting on anticoagulation prescription, thromboembolism, bleeding, and mortality. Anticoagulation rates and CHA<sub>2</sub>DS<sub>2</sub>-VASc scores were correlated, and a meta-analysis was conducted to compare short- and long-term outcomes.</p><p><strong>Results: </strong>Anticoagulation prescription rates ranged from 3 to 86%; in over 50% of patients, CHA<sub>2</sub>DS<sub>2</sub>-VASc scores were ≥ 2 (n = 28 studies). A meta-analysis of eight observational studies, in which 95% of patients had sepsis/infection as the precipitant, demonstrated no association between anticoagulation and reduced short-term thromboembolism (OR 0.89, 95% CI 0.61-1.28) or increased bleeding (OR 1.05, 95% CI 0.90-1.22). Short-term mortality was lower in the anticoagulation group (OR 0.54, 95% CI 0.39-0.75), but a higher long-term thromboembolic risk was observed (OR 1.45, 95% CI 1.04-2.03).</p><p><strong>Conclusion: </strong>The prescription of anticoagulation in critically ill patients with TIAF is highly variable. There is no clear evidence of benefit or harm, and neither routine use nor systematic omission is supported.</p>","PeriodicalId":18952,"journal":{"name":"Netherlands Heart Journal","volume":" ","pages":"290-298"},"PeriodicalIF":2.0000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454756/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Netherlands Heart Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12471-025-01978-9","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: In critically ill patients with trigger-induced atrial fibrillation, there are no definitive recommendations on the use of anticoagulation. This study aimed to evaluate the association between anticoagulation therapy and outcomes (i.e. thromboembolism, bleeding and mortality) and examine prescription patterns in high-risk individuals based on CHA2DS2-VASc scores.
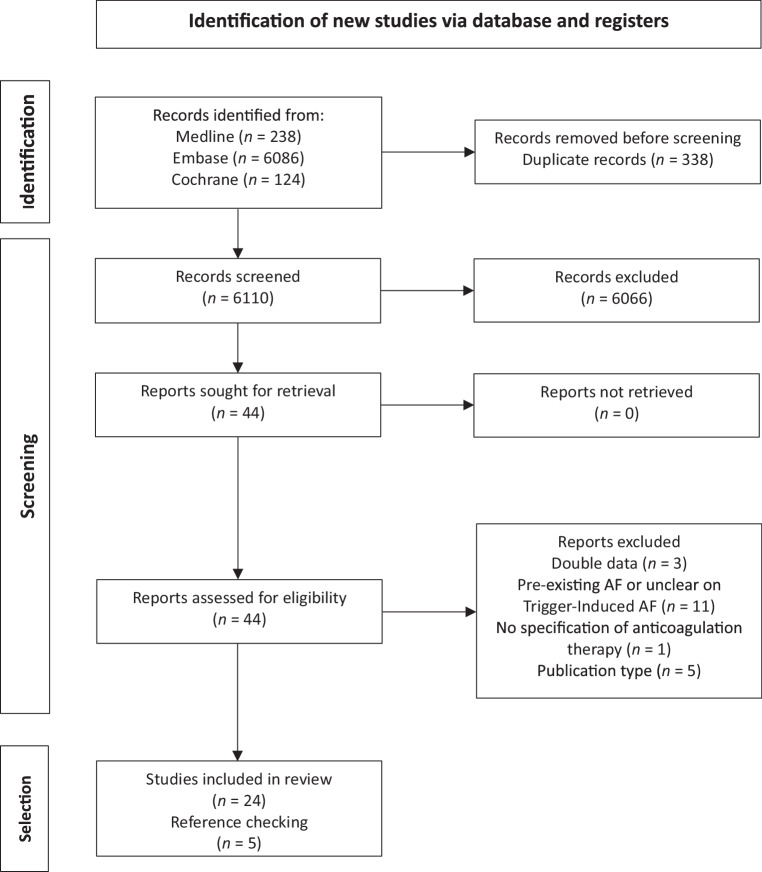
Methods: A systematic search was conducted to identify studies reporting on anticoagulation prescription, thromboembolism, bleeding, and mortality. Anticoagulation rates and CHA2DS2-VASc scores were correlated, and a meta-analysis was conducted to compare short- and long-term outcomes.
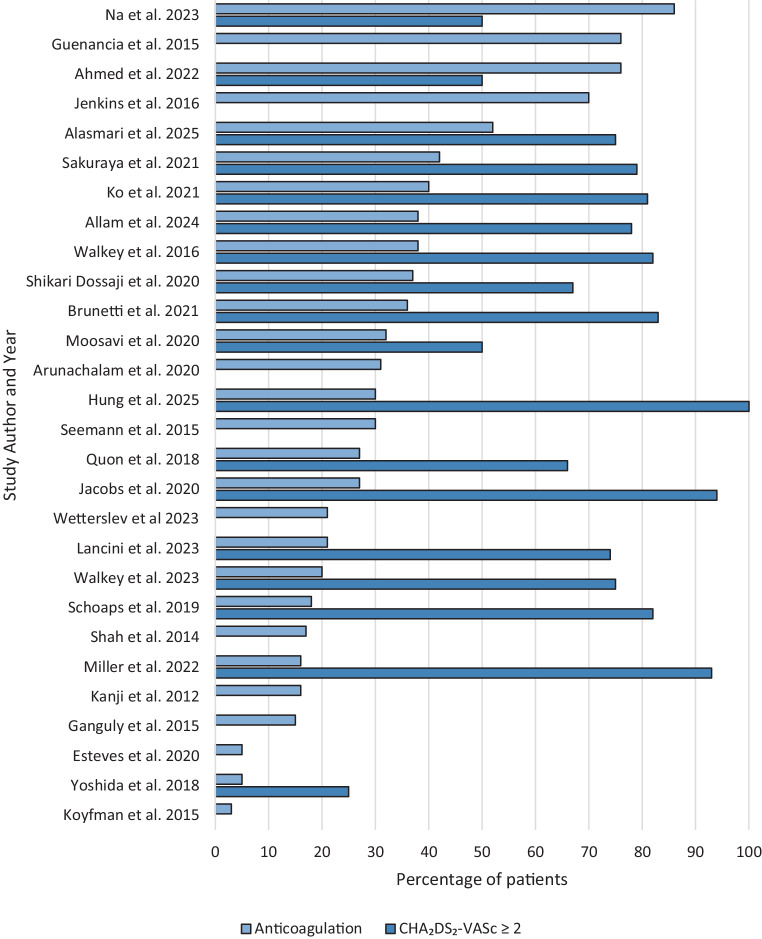
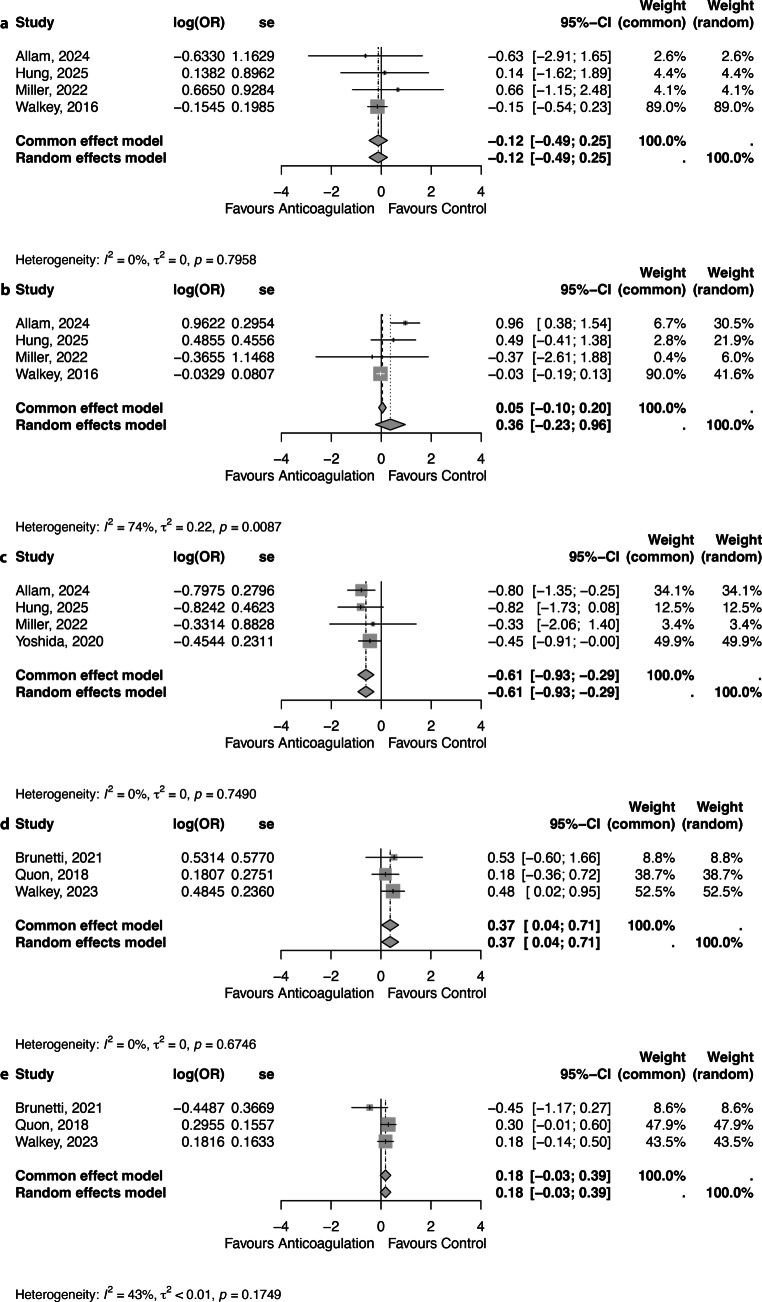
Results: Anticoagulation prescription rates ranged from 3 to 86%; in over 50% of patients, CHA2DS2-VASc scores were ≥ 2 (n = 28 studies). A meta-analysis of eight observational studies, in which 95% of patients had sepsis/infection as the precipitant, demonstrated no association between anticoagulation and reduced short-term thromboembolism (OR 0.89, 95% CI 0.61-1.28) or increased bleeding (OR 1.05, 95% CI 0.90-1.22). Short-term mortality was lower in the anticoagulation group (OR 0.54, 95% CI 0.39-0.75), but a higher long-term thromboembolic risk was observed (OR 1.45, 95% CI 1.04-2.03).
Conclusion: The prescription of anticoagulation in critically ill patients with TIAF is highly variable. There is no clear evidence of benefit or harm, and neither routine use nor systematic omission is supported.
期刊介绍:
The scope of the Netherlands Heart Journal is to contribute to the national and international literature by publishing scientific papers in the field of cardiovascular medicine. It also provides a platform for Continuing Medical Education for cardiologists and those in training for the speciality of cardiology in the Netherlands.
The Netherlands Heart Journal is made available to cardiologists, cardiologists in training, cardiopulmonary surgeons, cardiopulmonary surgeons in training, internists and paediatric cardiologists. The journal is the official journal of the Netherlands Society of Cardiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


