Factors and preventive strategies for perioperative euglycemic diabetic ketoacidosis in patients with type 2 diabetes receiving sodium-glucose cotransporter 2 inhibitors: a retrospective study.
{"title":"Factors and preventive strategies for perioperative euglycemic diabetic ketoacidosis in patients with type 2 diabetes receiving sodium-glucose cotransporter 2 inhibitors: a retrospective study.","authors":"Miho Takemura, Kenji Ikemura, Masahiro Okuda","doi":"10.1186/s40780-025-00487-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Invasive treatment and the associated stress are known risk factors for sodium-glucose cotransporter 2 inhibitor (SGLT2i)-induced euglycemic diabetic ketoacidosis (euDKA) development. It is recommended that SGLT2is is discontinued at least 3 days prior to a scheduled surgery. However, it is unclear whether preoperative discontinuation of SGLT2is is effective and whether other factors contribute to the development of SGLT2i-induced perioperative euDKA.</p><p><strong>Methods: </strong>We retrospectively investigated the incidence of euDKA postoperatively up to 30 days in patients receiving SGLT2is and undergoing surgery under general anesthesia. Multivariate logistic regression analysis was performed to identify the factors affecting euDKA development.</p><p><strong>Results: </strong>Twenty-one of 1,169 eligible patients (1.8%) developed perioperative euDKA. The incidence of perioperative euDKA in patients who discontinued SGLT2is for ≥ 3 days prior to surgery was significantly lower than that in patients who did not discontinue SGLT2is for ≥ 3 days prior to surgery (p < 0.001). The multivariate analysis showed that discontinuation of SGLT2is for ≥ 3 days prior to surgery and preoperative use of insulin and glucose infusion were significant factors that affected the development of perioperative euDKA (odds ratios = 0.047 and 0.054, p = 0.003 and 0.005, respectively).</p><p><strong>Conclusions: </strong>Our findings suggest that preoperative SGLT2i discontinuation for at least 3 days could prevent perioperative euDKA development and that preoperative insulin and glucose infusion could reduce the risk of developing euDKA, even in patients who cannot discontinue SGLT2is at least 3 days preoperatively.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"11 1","pages":"79"},"PeriodicalIF":1.2000,"publicationDate":"2025-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12376744/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-025-00487-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Invasive treatment and the associated stress are known risk factors for sodium-glucose cotransporter 2 inhibitor (SGLT2i)-induced euglycemic diabetic ketoacidosis (euDKA) development. It is recommended that SGLT2is is discontinued at least 3 days prior to a scheduled surgery. However, it is unclear whether preoperative discontinuation of SGLT2is is effective and whether other factors contribute to the development of SGLT2i-induced perioperative euDKA.
Methods: We retrospectively investigated the incidence of euDKA postoperatively up to 30 days in patients receiving SGLT2is and undergoing surgery under general anesthesia. Multivariate logistic regression analysis was performed to identify the factors affecting euDKA development.
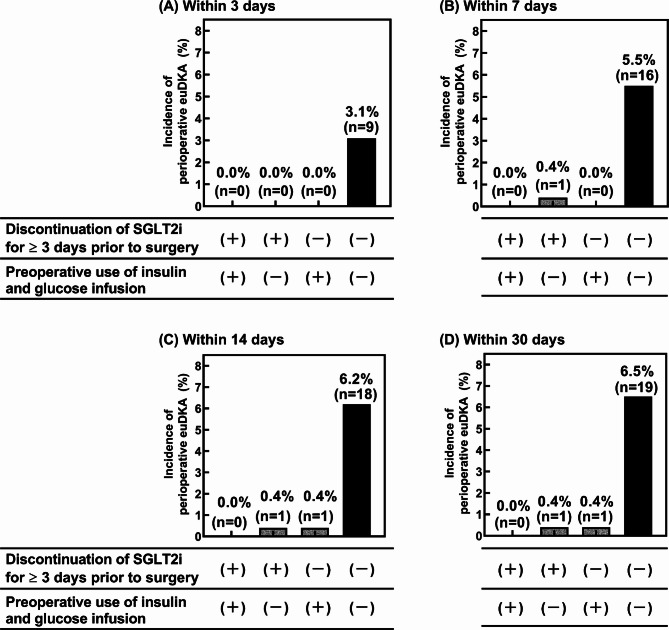
Results: Twenty-one of 1,169 eligible patients (1.8%) developed perioperative euDKA. The incidence of perioperative euDKA in patients who discontinued SGLT2is for ≥ 3 days prior to surgery was significantly lower than that in patients who did not discontinue SGLT2is for ≥ 3 days prior to surgery (p < 0.001). The multivariate analysis showed that discontinuation of SGLT2is for ≥ 3 days prior to surgery and preoperative use of insulin and glucose infusion were significant factors that affected the development of perioperative euDKA (odds ratios = 0.047 and 0.054, p = 0.003 and 0.005, respectively).
Conclusions: Our findings suggest that preoperative SGLT2i discontinuation for at least 3 days could prevent perioperative euDKA development and that preoperative insulin and glucose infusion could reduce the risk of developing euDKA, even in patients who cannot discontinue SGLT2is at least 3 days preoperatively.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


