{"title":"Anteroposterior Diameter Is Associated with Conversion from Right Minithoracotomy to Median Sternotomy in Minimally Invasive Cardiac Surgery.","authors":"Quynh Nguyen, Durr Al-Hakim, Richard C Cook","doi":"10.3390/jpm15080353","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: Minimally invasive cardiac surgery (MICS) via right minithoracotomy is a safe, reproducible approach with excellent outcomes and reduced costs compared to median sternotomy. Despite careful patient selection, conversion to sternotomy occurs in 1-3% of cases and is associated with significantly higher morbidity and mortality. Small body habitus, particularly a short anteroposterior (AP) diameter, may increase the risk of conversion, but this has not been previously studied. This study aims to identify preoperative factors associated with conversion to improve patient selection for MICS. As cardiovascular surgery becomes increasingly personalized, identifying anatomical factors that predict technical complexity is essential. <b>Methods</b>: This retrospective study included 254 adult patients who underwent elective MICS between 2015 and 2024 at a tertiary hospital. Patient characteristics, computed tomography (CT) scans, intraoperative parameters, and postoperative outcomes were reviewed. AP diameter was defined as the distance from the posterior sternum to the anterior vertebral body at the mitral valve level on CT. Statistical analyses included Mann-Whitney and Fisher's exact/chi-square tests. <b>Results</b>: Conversion to sternotomy occurred in 1.6% of patients (n = 4). All converted patients were female. The converted group had a significantly shorter median AP diameter (100 mm vs. 124 mm, <i>p</i> = 0.020). Conversion was associated with higher rates of stroke and infection (25.0% vs. 0.8%, <i>p</i> = 0.047 for both), but no significant differences in hospital stay, bleeding, or renal failure. <b>Conclusions:</b> An AP diameter of less than 100 mm was associated with a higher risk of conversion to sternotomy in MICS. Incorporating simple, reproducible preoperative imaging metrics into surgical planning may advance precision-guided cardiac surgery and optimize patient outcomes.</p>","PeriodicalId":16722,"journal":{"name":"Journal of Personalized Medicine","volume":"15 8","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387597/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Personalized Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jpm15080353","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
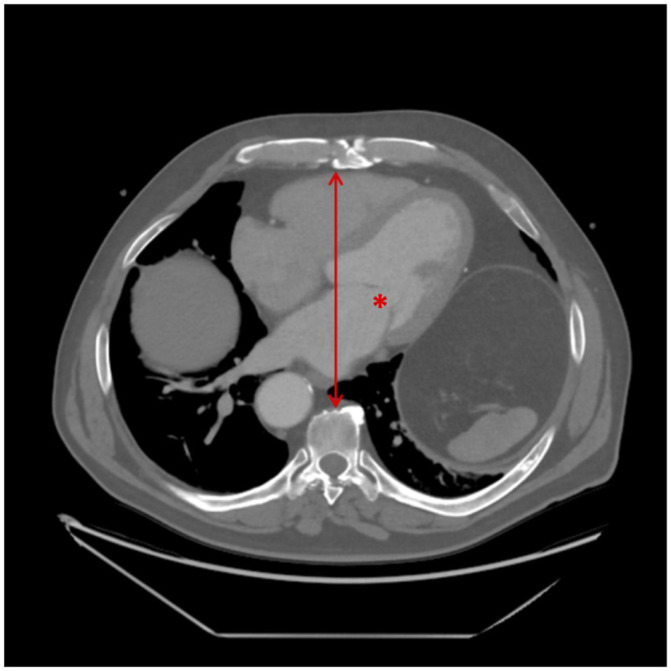
Background: Minimally invasive cardiac surgery (MICS) via right minithoracotomy is a safe, reproducible approach with excellent outcomes and reduced costs compared to median sternotomy. Despite careful patient selection, conversion to sternotomy occurs in 1-3% of cases and is associated with significantly higher morbidity and mortality. Small body habitus, particularly a short anteroposterior (AP) diameter, may increase the risk of conversion, but this has not been previously studied. This study aims to identify preoperative factors associated with conversion to improve patient selection for MICS. As cardiovascular surgery becomes increasingly personalized, identifying anatomical factors that predict technical complexity is essential. Methods: This retrospective study included 254 adult patients who underwent elective MICS between 2015 and 2024 at a tertiary hospital. Patient characteristics, computed tomography (CT) scans, intraoperative parameters, and postoperative outcomes were reviewed. AP diameter was defined as the distance from the posterior sternum to the anterior vertebral body at the mitral valve level on CT. Statistical analyses included Mann-Whitney and Fisher's exact/chi-square tests. Results: Conversion to sternotomy occurred in 1.6% of patients (n = 4). All converted patients were female. The converted group had a significantly shorter median AP diameter (100 mm vs. 124 mm, p = 0.020). Conversion was associated with higher rates of stroke and infection (25.0% vs. 0.8%, p = 0.047 for both), but no significant differences in hospital stay, bleeding, or renal failure. Conclusions: An AP diameter of less than 100 mm was associated with a higher risk of conversion to sternotomy in MICS. Incorporating simple, reproducible preoperative imaging metrics into surgical planning may advance precision-guided cardiac surgery and optimize patient outcomes.
期刊介绍:
Journal of Personalized Medicine (JPM; ISSN 2075-4426) is an international, open access journal aimed at bringing all aspects of personalized medicine to one platform. JPM publishes cutting edge, innovative preclinical and translational scientific research and technologies related to personalized medicine (e.g., pharmacogenomics/proteomics, systems biology). JPM recognizes that personalized medicine—the assessment of genetic, environmental and host factors that cause variability of individuals—is a challenging, transdisciplinary topic that requires discussions from a range of experts. For a comprehensive perspective of personalized medicine, JPM aims to integrate expertise from the molecular and translational sciences, therapeutics and diagnostics, as well as discussions of regulatory, social, ethical and policy aspects. We provide a forum to bring together academic and clinical researchers, biotechnology, diagnostic and pharmaceutical companies, health professionals, regulatory and ethical experts, and government and regulatory authorities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


