A case of adrenal insufficiency presenting with seizures, complicated by developmental cerebral venous anomaly and Takotsubo cardiomyopathy: a case report.
{"title":"A case of adrenal insufficiency presenting with seizures, complicated by developmental cerebral venous anomaly and Takotsubo cardiomyopathy: a case report.","authors":"Katrina Villegas, Brittany Eason, Karolina Janiec, Alaa Musallam, Ahmed Hammouda, Samia Ammar Aldwaik, Radhika Tailor","doi":"10.1186/s13256-025-05463-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adrenal insufficiency is a potentially life-threatening condition that often presents with nonspecific symptoms. While fatigue, hypotension, and electrolyte disturbances are common features, seizures and stress-induced cardiomyopathy are rare initial manifestations. This case is reported for its atypical presentation and to highlight the diagnostic challenge it posed in the absence of classic biochemical findings.</p><p><strong>Case presentation: </strong>We report a case of a 68-year-old Hispanic woman with diabetes, hypertension, dyslipidemia, and hypopituitarism secondary to Sheehan syndrome, who presented with new-onset seizures after abruptly discontinuing chronic steroid therapy. Her symptoms included progressive weakness and behavioral changes over several weeks. Initial evaluation revealed hyperglycemia, mild hyponatremia, and no hyperkalemia-findings consistent with secondary adrenal insufficiency-associated seizures, although contributing to initial diagnostic uncertainty. Brain imaging incidentally identified a developmental cerebral venous anomaly, which was initially suspected as a potential cause of the seizures. In addition, echocardiographic findings were consistent with Takotsubo cardiomyopathy, likely precipitated by the stress of her medical condition. However, further evaluation confirmed adrenal insufficiency with low cortisol and adrenocorticotropic hormone levels, and subnormal response to cosyntropin stimulation. Management included hydrocortisone for adrenal insufficiency and levetiracetam for seizure prophylaxis, leading to symptom resolution and no recurrence of seizures.</p><p><strong>Conclusion: </strong>This case emphasizes the importance of maintaining a high index of suspicion for adrenal insufficiency in patients with a suggestive history, even when classic electrolyte abnormalities are absent and neuroimaging reveals confounding findings. Recognizing rare presentations such as seizures and stress cardiomyopathy can prevent delays in diagnosis and improve outcomes.</p>","PeriodicalId":16236,"journal":{"name":"Journal of Medical Case Reports","volume":"19 1","pages":"424"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372403/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13256-025-05463-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adrenal insufficiency is a potentially life-threatening condition that often presents with nonspecific symptoms. While fatigue, hypotension, and electrolyte disturbances are common features, seizures and stress-induced cardiomyopathy are rare initial manifestations. This case is reported for its atypical presentation and to highlight the diagnostic challenge it posed in the absence of classic biochemical findings.
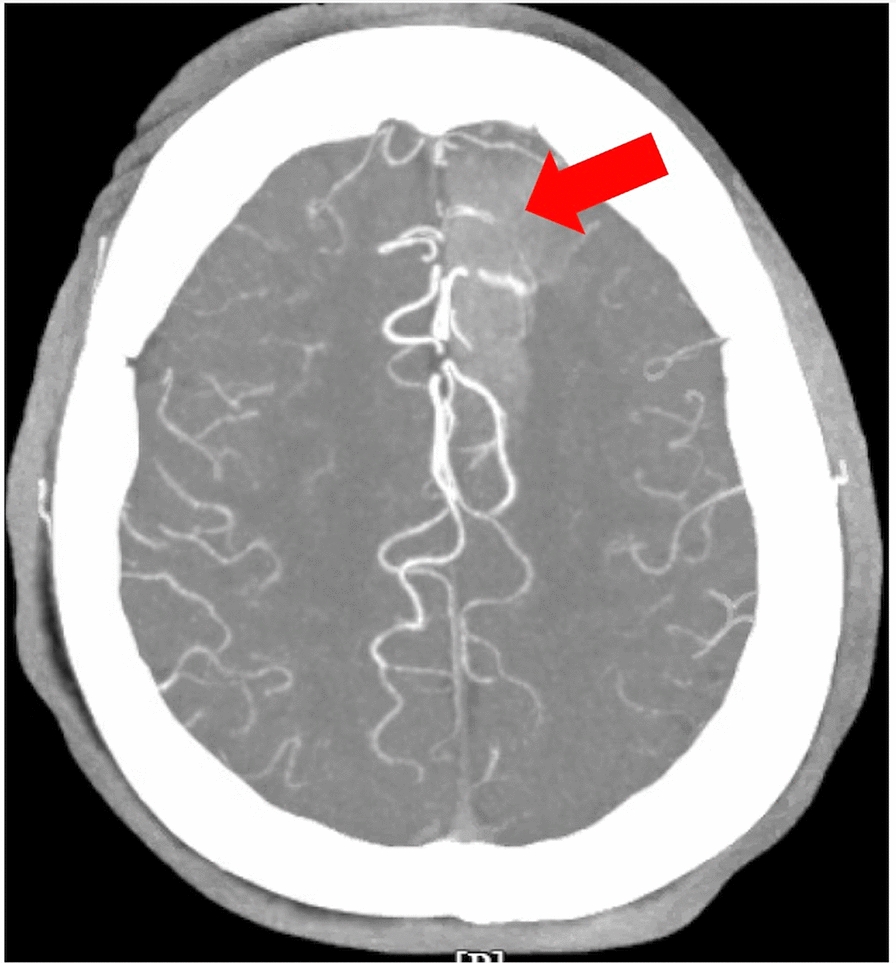
Case presentation: We report a case of a 68-year-old Hispanic woman with diabetes, hypertension, dyslipidemia, and hypopituitarism secondary to Sheehan syndrome, who presented with new-onset seizures after abruptly discontinuing chronic steroid therapy. Her symptoms included progressive weakness and behavioral changes over several weeks. Initial evaluation revealed hyperglycemia, mild hyponatremia, and no hyperkalemia-findings consistent with secondary adrenal insufficiency-associated seizures, although contributing to initial diagnostic uncertainty. Brain imaging incidentally identified a developmental cerebral venous anomaly, which was initially suspected as a potential cause of the seizures. In addition, echocardiographic findings were consistent with Takotsubo cardiomyopathy, likely precipitated by the stress of her medical condition. However, further evaluation confirmed adrenal insufficiency with low cortisol and adrenocorticotropic hormone levels, and subnormal response to cosyntropin stimulation. Management included hydrocortisone for adrenal insufficiency and levetiracetam for seizure prophylaxis, leading to symptom resolution and no recurrence of seizures.
Conclusion: This case emphasizes the importance of maintaining a high index of suspicion for adrenal insufficiency in patients with a suggestive history, even when classic electrolyte abnormalities are absent and neuroimaging reveals confounding findings. Recognizing rare presentations such as seizures and stress cardiomyopathy can prevent delays in diagnosis and improve outcomes.
期刊介绍:
JMCR is an open access, peer-reviewed online journal that will consider any original case report that expands the field of general medical knowledge. Reports should show one of the following: 1. Unreported or unusual side effects or adverse interactions involving medications 2. Unexpected or unusual presentations of a disease 3. New associations or variations in disease processes 4. Presentations, diagnoses and/or management of new and emerging diseases 5. An unexpected association between diseases or symptoms 6. An unexpected event in the course of observing or treating a patient 7. Findings that shed new light on the possible pathogenesis of a disease or an adverse effect

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


