Sinus Tachycardia and Unrelieved Wall Stress Precede Left Ventricular Systolic Dysfunction During Preclinical Cardiomyopathic Changes in Duchenne Muscular Dystrophy.
{"title":"Sinus Tachycardia and Unrelieved Wall Stress Precede Left Ventricular Systolic Dysfunction During Preclinical Cardiomyopathic Changes in Duchenne Muscular Dystrophy.","authors":"Takeshi Tsuda, Amy Walczak, Karen O'Neil","doi":"10.3390/jcdd12080280","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The onset of cardiomyopathy in Duchenne muscular dystrophy (DMD) is insidious and poorly defined. We proposed integrated wall stress (iWS) as a marker of total left ventricular (LV) workload and tested whether the increased iWS represents early DMD cardiomyopathy.</p><p><strong>Methods: </strong>Peak systolic wall stress (PS-WS) was calculated in M-mode echocardiography with simultaneous blood pressure measurement. iWS was defined as a product of PS-WS and heart rate (HR) divided by 60 (=PS-WS/RR interval). We measured iWS in normal controls (CTRL), DMD with normal LV shortening fraction (%LVSF ≥ 30%) (DMD-A), and DMD with decreased %LVSF (<30%) (DMD-B).</p><p><strong>Results: </strong>40 CTRL and 79 DMD patients were studied. Despite comparable %LVSF, both HR and iWS were significantly higher in DMD-A (n = 50) than in CTRL (<i>p</i> < 0.0001). iWS was significantly higher in DMD-B (n = 29) than in DMD-A (<i>p</i> < 0.0001) despite comparable HR. PS-WS was significantly higher in DMD-A than in CTRL and higher in DMD-B than in DMD-A, suggesting high HR is not a sole determinant of increased iWS in DMD-A compared with CTRL. In a longitudinal study in 35 DMD patients over 4.0 ± 2.0 years, iWS showed significant increase (<i>p</i> = 0.0062) alongside a significant decline in %LVSF (<i>p</i> < 0.0001).</p><p><strong>Conclusions: </strong>iWS significantly increased in DMD before %LVSF declined. The progressive increase of iWS in DMD is initially associated with increased HR and then with increased PS-WS. iWS may serve as a useful echocardiographic marker in identifying preclinical DMD cardiomyopathy.</p>","PeriodicalId":15197,"journal":{"name":"Journal of Cardiovascular Development and Disease","volume":"12 8","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12387109/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Development and Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcdd12080280","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The onset of cardiomyopathy in Duchenne muscular dystrophy (DMD) is insidious and poorly defined. We proposed integrated wall stress (iWS) as a marker of total left ventricular (LV) workload and tested whether the increased iWS represents early DMD cardiomyopathy.
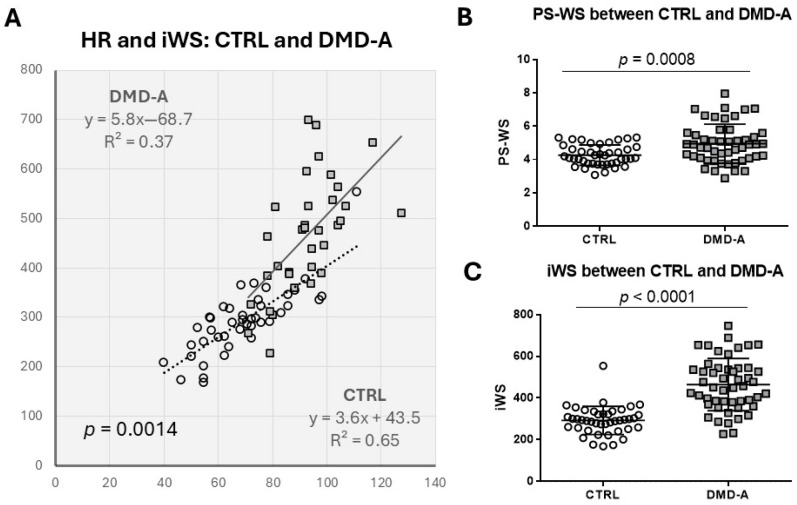
Methods: Peak systolic wall stress (PS-WS) was calculated in M-mode echocardiography with simultaneous blood pressure measurement. iWS was defined as a product of PS-WS and heart rate (HR) divided by 60 (=PS-WS/RR interval). We measured iWS in normal controls (CTRL), DMD with normal LV shortening fraction (%LVSF ≥ 30%) (DMD-A), and DMD with decreased %LVSF (<30%) (DMD-B).
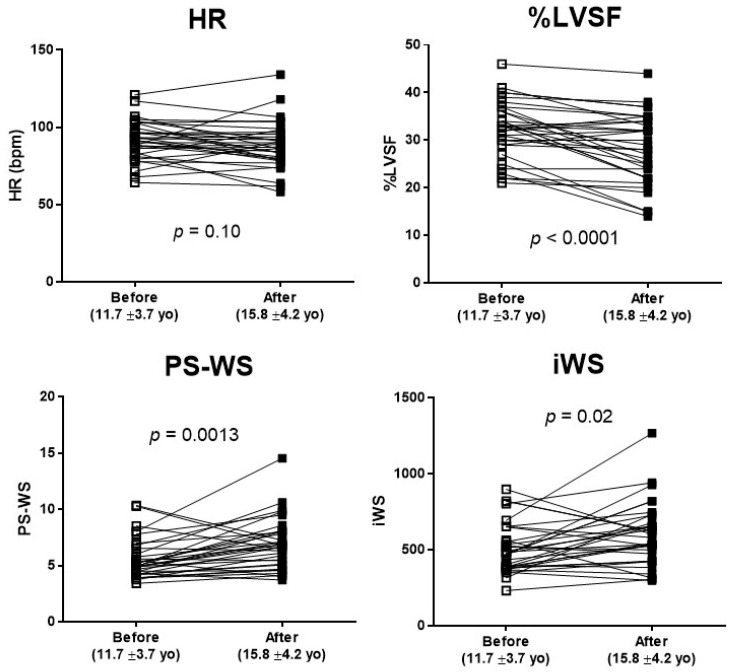
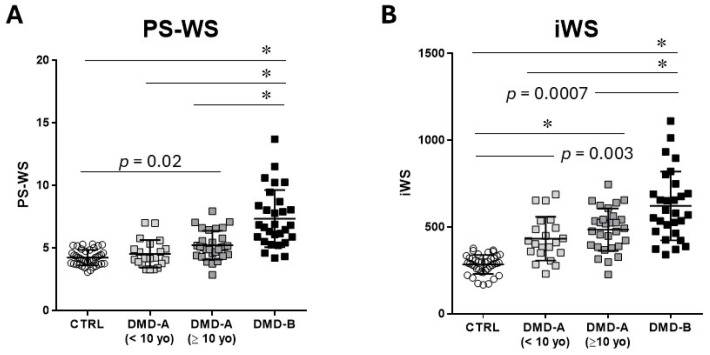
Results: 40 CTRL and 79 DMD patients were studied. Despite comparable %LVSF, both HR and iWS were significantly higher in DMD-A (n = 50) than in CTRL (p < 0.0001). iWS was significantly higher in DMD-B (n = 29) than in DMD-A (p < 0.0001) despite comparable HR. PS-WS was significantly higher in DMD-A than in CTRL and higher in DMD-B than in DMD-A, suggesting high HR is not a sole determinant of increased iWS in DMD-A compared with CTRL. In a longitudinal study in 35 DMD patients over 4.0 ± 2.0 years, iWS showed significant increase (p = 0.0062) alongside a significant decline in %LVSF (p < 0.0001).
Conclusions: iWS significantly increased in DMD before %LVSF declined. The progressive increase of iWS in DMD is initially associated with increased HR and then with increased PS-WS. iWS may serve as a useful echocardiographic marker in identifying preclinical DMD cardiomyopathy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


