{"title":"Electrophysiological Substrate and Pulmonary Vein Reconnection Patterns in Recurrent Atrial Fibrillation: Comparing Thermal Strategies in Patients Undergoing Redo Ablation.","authors":"Krisztian Istvan Kassa, Adwity Shakya, Zoltan Som, Csaba Foldesi, Attila Kardos","doi":"10.3390/jcdd12080298","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The influence of the initial ablation modality on pulmonary vein (PV) reconnection and substrate characteristics in redo procedures for recurrent atrial fibrillation (AF) remains unclear. We assessed how different thermal strategies-ablation index (AI)-guided radiofrequency (RF) versus cryoballoon (CB) ablation-affect remapping findings during redo pulmonary vein isolation (PVI).</p><p><strong>Methods: </strong>We included patients undergoing redo ablation between 2015 and 2024 with high-density electroanatomic mapping. Initial PVI modalities were retrospectively classified as low-power, long-duration (LPLD) RF; high-power, short-duration (HPSD) RF; or second-/third-generation CB. Reconnection sites were mapped using multielectrode catheters. Redo PVI was performed using AI-guided RF. Segments showing PV reconnection were reisolated; if all PVs remained isolated and AF persisted, posterior wall isolation was performed.</p><p><strong>Results: </strong>Among 195 patients (LPLD: 63; HPSD: 30; CB: 102), complete PVI at redo was observed in 0% (LPLD), 23.3% (HPSD), and 10.1% (CB) (<i>p</i> < 0.01 for LPLD vs. HPSD). Reconnection patterns varied by technique; LPLD primarily affected the right carina, while HPSD and CB showed reconnections at the LSPV ridge. Organized atrial tachycardia was least frequent after CB (12.7%, <i>p</i> < 0.002).</p><p><strong>Conclusion: </strong>Initial ablation strategy significantly influences PV reconnection and post-PVI arrhythmia patterns, with implications for redo procedure planning.</p>","PeriodicalId":15197,"journal":{"name":"Journal of Cardiovascular Development and Disease","volume":"12 8","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386683/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Development and Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcdd12080298","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The influence of the initial ablation modality on pulmonary vein (PV) reconnection and substrate characteristics in redo procedures for recurrent atrial fibrillation (AF) remains unclear. We assessed how different thermal strategies-ablation index (AI)-guided radiofrequency (RF) versus cryoballoon (CB) ablation-affect remapping findings during redo pulmonary vein isolation (PVI).
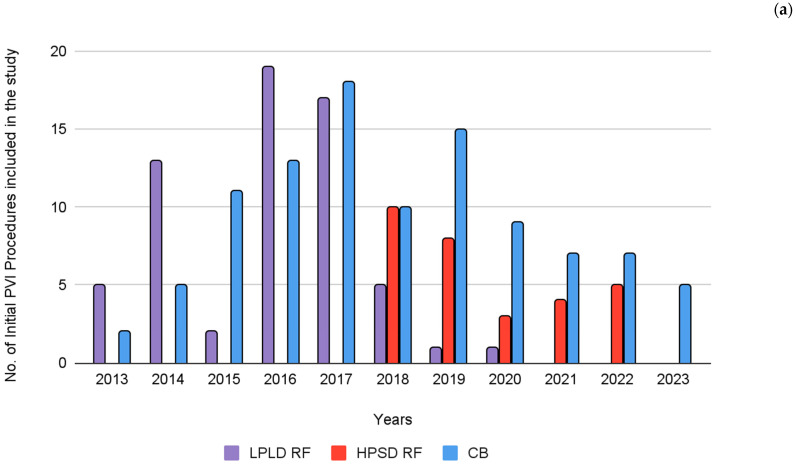
Methods: We included patients undergoing redo ablation between 2015 and 2024 with high-density electroanatomic mapping. Initial PVI modalities were retrospectively classified as low-power, long-duration (LPLD) RF; high-power, short-duration (HPSD) RF; or second-/third-generation CB. Reconnection sites were mapped using multielectrode catheters. Redo PVI was performed using AI-guided RF. Segments showing PV reconnection were reisolated; if all PVs remained isolated and AF persisted, posterior wall isolation was performed.
Results: Among 195 patients (LPLD: 63; HPSD: 30; CB: 102), complete PVI at redo was observed in 0% (LPLD), 23.3% (HPSD), and 10.1% (CB) (p < 0.01 for LPLD vs. HPSD). Reconnection patterns varied by technique; LPLD primarily affected the right carina, while HPSD and CB showed reconnections at the LSPV ridge. Organized atrial tachycardia was least frequent after CB (12.7%, p < 0.002).
Conclusion: Initial ablation strategy significantly influences PV reconnection and post-PVI arrhythmia patterns, with implications for redo procedure planning.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


