Luca Attisani, Alessandro Pucci, Matteo A Pegorer, Luca Luzzani, Francesco Casali, Giorgio Luoni, Stefano Tanagli, Gabriele Piffaretti, Raffaello Bellosta
{"title":"Clinical Outcomes of Surgical Revascularization in Patients Presenting with Critical Limb Ischemia and Aortic Valve Stenosis.","authors":"Luca Attisani, Alessandro Pucci, Matteo A Pegorer, Luca Luzzani, Francesco Casali, Giorgio Luoni, Stefano Tanagli, Gabriele Piffaretti, Raffaello Bellosta","doi":"10.3390/jcdd12080292","DOIUrl":null,"url":null,"abstract":"<p><p>(1) Background: Comparison of clinical outcomes between patients with moderate-severe aortic valve stenosis and those with mild or no aortic valve stenosis undergoing surgical revascularization for critical limb threating ischemia (CLTI). (2) Methods: Single center retrospective analysis of consecutive patients undergoing surgical lower limb revascularization with femoro-distal bypass for critical ischemia between 2016 and 2022. All patients were evaluated preoperatively by echocardiographic examination and divided into two cohorts: group A with moderate-severe aortic valve stenosis (AVA-cm<sup>2</sup> < or =1.5 cm<sup>2</sup>) and group B with mild or absent stenosis (AVA-cm<sup>2</sup> > 1.5 cm<sup>2</sup>). Primary outcomes were major limb amputation and mortality between the two groups. The rate of major cardiovascular events (stroke, myocardial infarction, sudden cardiac death) and change in \"preoperative functional status\" were the secondary outcomes. Descriptive statistics for continuous variables were performed by calculating means, standard deviation (SD) medians, and interquartile range (IQR) while, for categorical variables, frequencies and percentages were performed. Intergroup comparison tests, for continuous variables, were performed by <i>t</i>-test or corresponding nonparametric tests (Mann-Whitney test) while, for categorical variables, Chi-square test was used. Evaluation of cut-offs for the variable AVA-fx-cm<sup>2</sup>, in terms of predictive of outcome outcomes, was calculated by ROC curves. Comparison between clinical and outcome variables was performed using logistic regression models. A total of 316 patients were analyzed and divided in two groups: 50 (16%) patients with moderate or severe aortic valve stenosis (group A) and 266 (84%) with no or mild aortic valve stenosis (AVA > 1.5 cm<sup>2</sup>). Patients in group A were significantly older than those in group B (78 years vs. 74 years, <i>p</i> value = 0.005); no other significant comorbidity differences were found between the two groups. The mean follow-up was 1178 days (SD 991 days; 2-3869 days). There were no statistically significant differences between group A and group B in terms of major amputation rate (20% vs. 16.5%; <i>p</i> = 0.895) and overall mortality (48.0% vs. 40.6%; <i>p</i> = 0.640). In the total cohort, the statistically significant variables associated with the major amputation were systemic perioperative complication (OR 5.83, 95% CI: 2.36, 14.57, <i>p</i> < 0.001), bypass-related complication within 30 days of surgery (OR 2.74, 95% CI: 1.17, 6.45, <i>p</i> = 0.020), surgical revascularization below the knee (OR 7.72, 95% CI: 1.53, 140.68, <i>p</i> = 0.049), and the presence of a previous cardiovascular event (OR 2.65, 95% CI: 1.14, 6.26, <i>p</i> = 0.024). In patients undergoing surgical revascularization for CLTI, no significant difference in major amputation rate and overall mortality was found between subjects with mild or no aortic valve stenosis and those with moderate/severe stenosis. As expected, overall mortality was higher in older patients with worse functional status. A significantly higher rate of limb amputation was found in those subjects undergoing subgenicular revascularization, early bypass failure, or previous cardiovascular event.</p>","PeriodicalId":15197,"journal":{"name":"Journal of Cardiovascular Development and Disease","volume":"12 8","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386372/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Development and Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcdd12080292","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
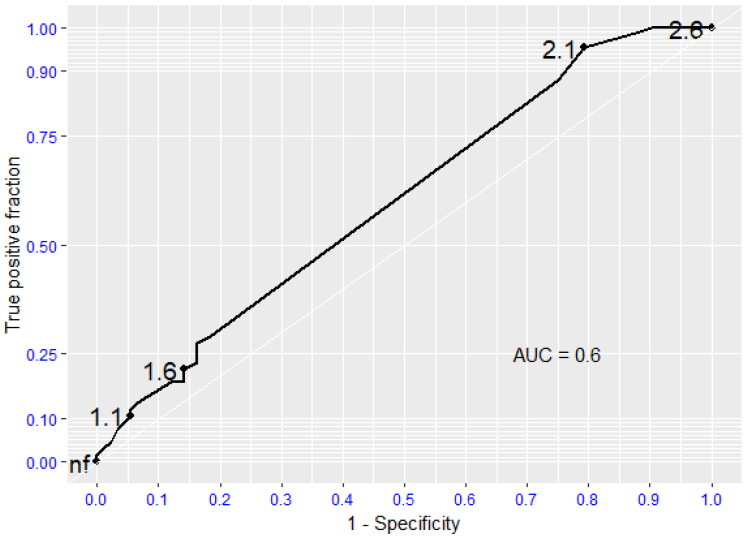
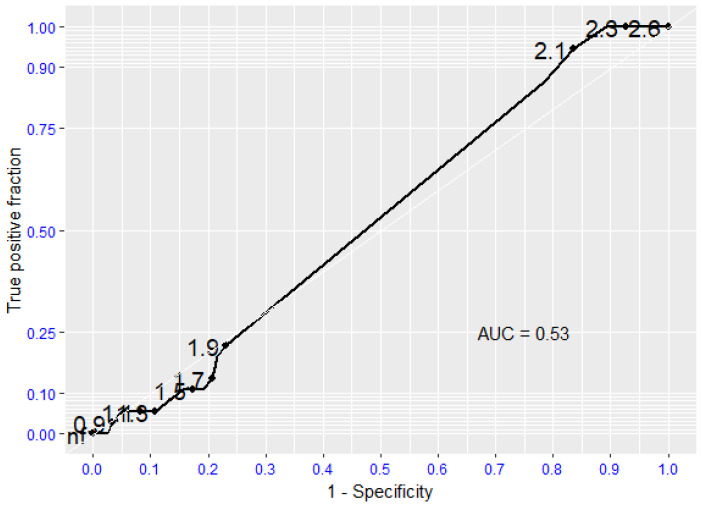
(1) Background: Comparison of clinical outcomes between patients with moderate-severe aortic valve stenosis and those with mild or no aortic valve stenosis undergoing surgical revascularization for critical limb threating ischemia (CLTI). (2) Methods: Single center retrospective analysis of consecutive patients undergoing surgical lower limb revascularization with femoro-distal bypass for critical ischemia between 2016 and 2022. All patients were evaluated preoperatively by echocardiographic examination and divided into two cohorts: group A with moderate-severe aortic valve stenosis (AVA-cm2 < or =1.5 cm2) and group B with mild or absent stenosis (AVA-cm2 > 1.5 cm2). Primary outcomes were major limb amputation and mortality between the two groups. The rate of major cardiovascular events (stroke, myocardial infarction, sudden cardiac death) and change in "preoperative functional status" were the secondary outcomes. Descriptive statistics for continuous variables were performed by calculating means, standard deviation (SD) medians, and interquartile range (IQR) while, for categorical variables, frequencies and percentages were performed. Intergroup comparison tests, for continuous variables, were performed by t-test or corresponding nonparametric tests (Mann-Whitney test) while, for categorical variables, Chi-square test was used. Evaluation of cut-offs for the variable AVA-fx-cm2, in terms of predictive of outcome outcomes, was calculated by ROC curves. Comparison between clinical and outcome variables was performed using logistic regression models. A total of 316 patients were analyzed and divided in two groups: 50 (16%) patients with moderate or severe aortic valve stenosis (group A) and 266 (84%) with no or mild aortic valve stenosis (AVA > 1.5 cm2). Patients in group A were significantly older than those in group B (78 years vs. 74 years, p value = 0.005); no other significant comorbidity differences were found between the two groups. The mean follow-up was 1178 days (SD 991 days; 2-3869 days). There were no statistically significant differences between group A and group B in terms of major amputation rate (20% vs. 16.5%; p = 0.895) and overall mortality (48.0% vs. 40.6%; p = 0.640). In the total cohort, the statistically significant variables associated with the major amputation were systemic perioperative complication (OR 5.83, 95% CI: 2.36, 14.57, p < 0.001), bypass-related complication within 30 days of surgery (OR 2.74, 95% CI: 1.17, 6.45, p = 0.020), surgical revascularization below the knee (OR 7.72, 95% CI: 1.53, 140.68, p = 0.049), and the presence of a previous cardiovascular event (OR 2.65, 95% CI: 1.14, 6.26, p = 0.024). In patients undergoing surgical revascularization for CLTI, no significant difference in major amputation rate and overall mortality was found between subjects with mild or no aortic valve stenosis and those with moderate/severe stenosis. As expected, overall mortality was higher in older patients with worse functional status. A significantly higher rate of limb amputation was found in those subjects undergoing subgenicular revascularization, early bypass failure, or previous cardiovascular event.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


