Hannah Wozniak, Eleonora Balzani, Vladimir Lazarevic, Nadia Gaia, Aude de Watteville, Raphaël Giraud, Jacques Schrenzel, Claudia Heidegger
{"title":"Gut microbiota differs between ICU patients admitted for cardiac arrest and other causes: a secondary, propensity-matched cohort analysis.","authors":"Hannah Wozniak, Eleonora Balzani, Vladimir Lazarevic, Nadia Gaia, Aude de Watteville, Raphaël Giraud, Jacques Schrenzel, Claudia Heidegger","doi":"10.1186/s40635-025-00803-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Critical illness is known to reduce gut microbiota (GM) diversity, a change associated with adverse outcomes. Among potential mechanisms, splanchnic hypoperfusion may play a key role. Cardiac arrest (CA), characterized by transient global hypoperfusion, provides a relevant model to explore this effect.</p><p><strong>Results: </strong>We conducted a secondary, propensity score-matched analysis of a cohort study investigating GM changes during early intensive care unit stay. Stool samples were collected at ICU admission (S1) and at least 24 h later (S2). GM profiling was performed using 16S rRNA sequencing. Shannon diversity index and taxonomic composition were compared between CA and non-CA patients. Propensity score matching and generalized linear models (GLM) were used to adjust for confounding. A total of 26 patients were included in this analysis (13 CA, 13 matched controls). At S1, CA patients had significantly lower GM diversity (Shannon index: 3.6 [3.0-3.8] vs. 4.3 [3.9-4.8], p = 0.019). This was confirmed in the GLM (β = - 0.30, SE 0.12, p = 0.022). At S2, diversity remained lower (3.2 [2.7-3.8] vs. 4.0 [3.7-4.3], p = 0.064). While no global compositional shifts were observed between groups, differences in the abundance of specific taxa were noted.</p><p><strong>Conclusion: </strong>CA is associated with reduced GM diversity in the first few days of intensive care unit admission compared to non-CA patients, supporting a role for splanchnic hypoperfusion in GM modulation. Further research should investigate clinical consequences and evaluate microbiota-targeted interventions in this high-risk population.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"88"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394093/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00803-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Critical illness is known to reduce gut microbiota (GM) diversity, a change associated with adverse outcomes. Among potential mechanisms, splanchnic hypoperfusion may play a key role. Cardiac arrest (CA), characterized by transient global hypoperfusion, provides a relevant model to explore this effect.
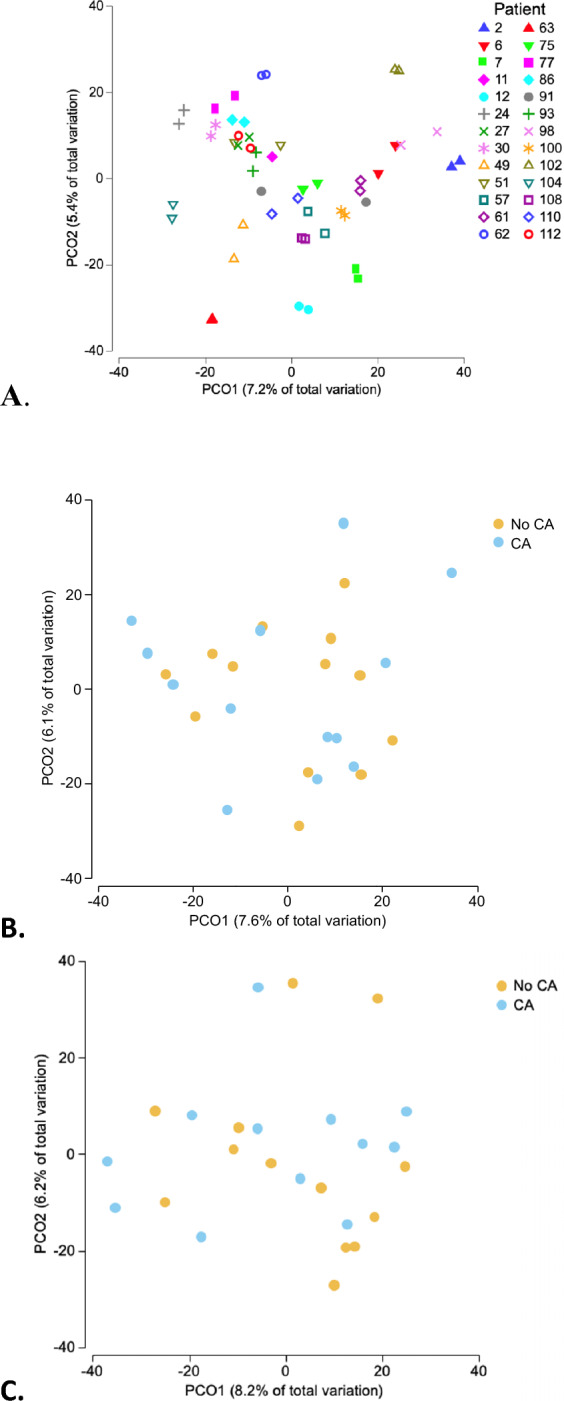
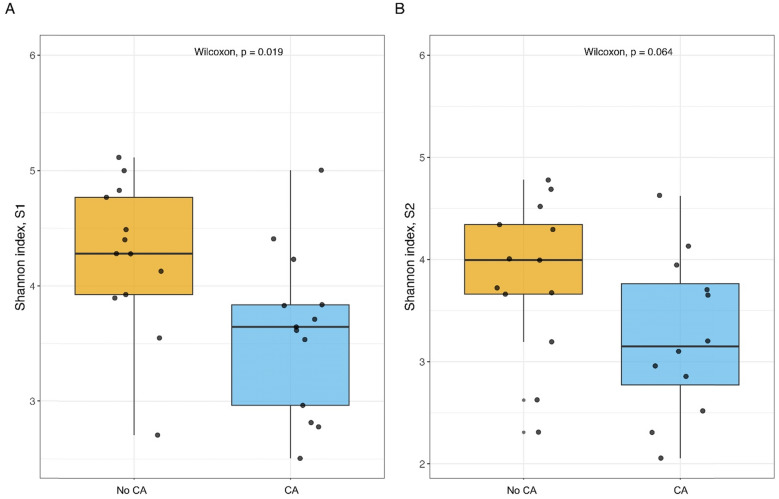
Results: We conducted a secondary, propensity score-matched analysis of a cohort study investigating GM changes during early intensive care unit stay. Stool samples were collected at ICU admission (S1) and at least 24 h later (S2). GM profiling was performed using 16S rRNA sequencing. Shannon diversity index and taxonomic composition were compared between CA and non-CA patients. Propensity score matching and generalized linear models (GLM) were used to adjust for confounding. A total of 26 patients were included in this analysis (13 CA, 13 matched controls). At S1, CA patients had significantly lower GM diversity (Shannon index: 3.6 [3.0-3.8] vs. 4.3 [3.9-4.8], p = 0.019). This was confirmed in the GLM (β = - 0.30, SE 0.12, p = 0.022). At S2, diversity remained lower (3.2 [2.7-3.8] vs. 4.0 [3.7-4.3], p = 0.064). While no global compositional shifts were observed between groups, differences in the abundance of specific taxa were noted.
Conclusion: CA is associated with reduced GM diversity in the first few days of intensive care unit admission compared to non-CA patients, supporting a role for splanchnic hypoperfusion in GM modulation. Further research should investigate clinical consequences and evaluate microbiota-targeted interventions in this high-risk population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


