{"title":"Evaluation of Altered Myocardial Blood Flow and Cardiovascular Function in Patients With Thyroid Cancer and Related Treatments.","authors":"Daniel Hueng-Yuan Shen, Hung-Pin Chan, Chin Hu, Wen-Hwa Wang, Yu-Li Chiu, Fu-Ren Tsai","doi":"10.21873/invivo.14092","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>This study aimed to explore changes in cardiovascular performance among patients with thyroid cancer following thyroidectomy, radioiodine therapy (RAIT) and thyroid-stimulating hormone suppression therapy (TST), with or without treatment with tyrosine kinase inhibitors (TKIs).</p><p><strong>Patients and methods: </strong>We enrolled 32 patients who underwent thyroidectomy and subsequent RAIT (except for one patient who underwent partial thyroidectomy only) and TST, with or without TKI therapy. We assessed myocardial perfusion using quantitative myocardial perfusion imaging (qMPI), myocardial blood flow (MBF), and coronary flow reserve (CFR) <i>via</i> dynamic single photon-emission computed tomography/computer tomography. We also analyzed data from laboratory tests or heart-related circulation markers, such as <i>N</i>-terminal pro B-type natriuretic peptide (NT-proBNP) to compare patient results, including correlations with different TKIs, RAIT, and TST.</p><p><strong>Results: </strong>qMPI indicated that the TKI-treated group (n=19) exhibited reduced MBF, CFR, and coronary flow capacity compared to the non-TKI-treated group. The right coronary artery (RCA) territory was notably affected by TKI treatment, particularly during the stress phase: RCA-stress blood flow: 2.4±0.6 <i>vs.</i> 1.9±0.7 ml/min/g; RCA-CFR: 2.3±0.8 <i>vs.</i> 2.93±0.9 for TKI-treated <i>vs.</i> non TKI-treated groups, respectively. This effect was more pronounced in the subgroup undergoing sequential anti-vascular endothelial growth factor TKI treatment (<i>e.g.</i> sorafenib and lenvatinib) (n=4) compared to non-TKI-treated controls. Additionally, TKI-treated patients showed a higher mean NT-ProBNP level (203±322.2 pg/ml) than non-TKI-treated patients (39.1±36 pg/ml). Abnormal MBF/CFR was also associated with higher cumulative RAIT dose and lower thyrotropin level.</p><p><strong>Conclusion: </strong>TKI therapy, especially anti-vascular endothelial growth factor TKI, can negatively affect myocardial perfusion and lead to coronary microcirculation dysfunction, reducing MBF/CFR during the stress phase. The link between cumulative RAIT dose, lower thyroid-stimulating hormone level, and abnormal MBF/CFR highlights the need for further research.</p>","PeriodicalId":13364,"journal":{"name":"In vivo","volume":"39 5","pages":"2919-2930"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396053/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"In vivo","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21873/invivo.14092","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aim: This study aimed to explore changes in cardiovascular performance among patients with thyroid cancer following thyroidectomy, radioiodine therapy (RAIT) and thyroid-stimulating hormone suppression therapy (TST), with or without treatment with tyrosine kinase inhibitors (TKIs).
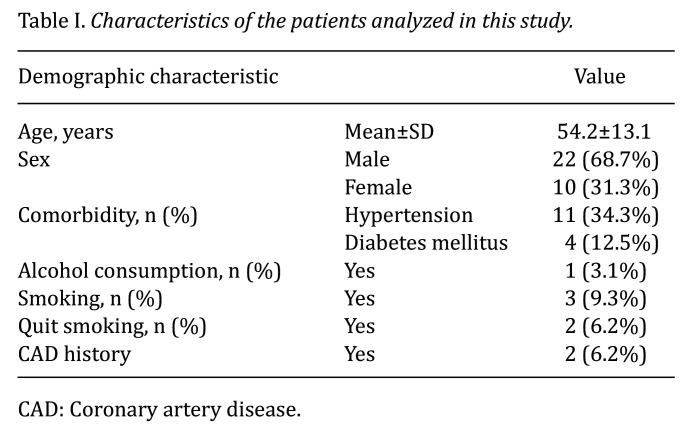
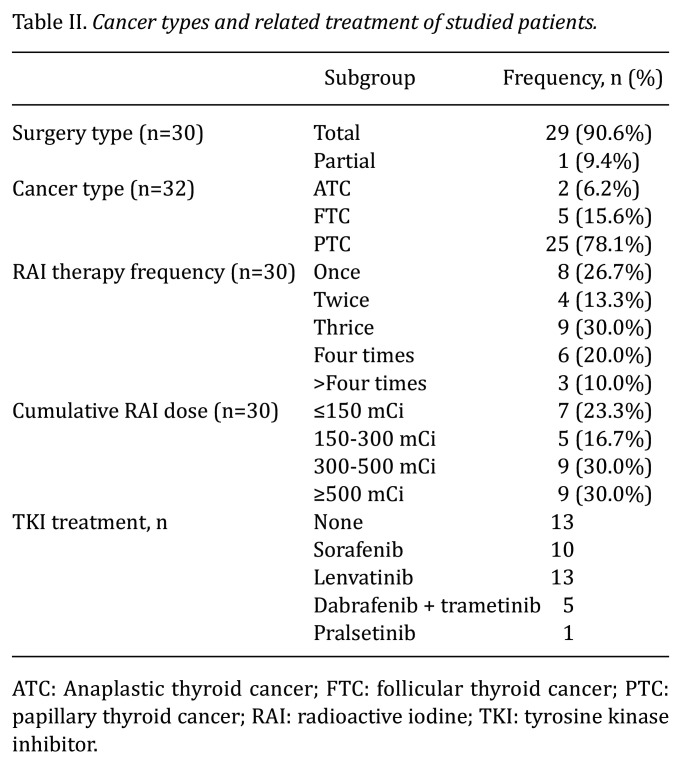
Patients and methods: We enrolled 32 patients who underwent thyroidectomy and subsequent RAIT (except for one patient who underwent partial thyroidectomy only) and TST, with or without TKI therapy. We assessed myocardial perfusion using quantitative myocardial perfusion imaging (qMPI), myocardial blood flow (MBF), and coronary flow reserve (CFR) via dynamic single photon-emission computed tomography/computer tomography. We also analyzed data from laboratory tests or heart-related circulation markers, such as N-terminal pro B-type natriuretic peptide (NT-proBNP) to compare patient results, including correlations with different TKIs, RAIT, and TST.
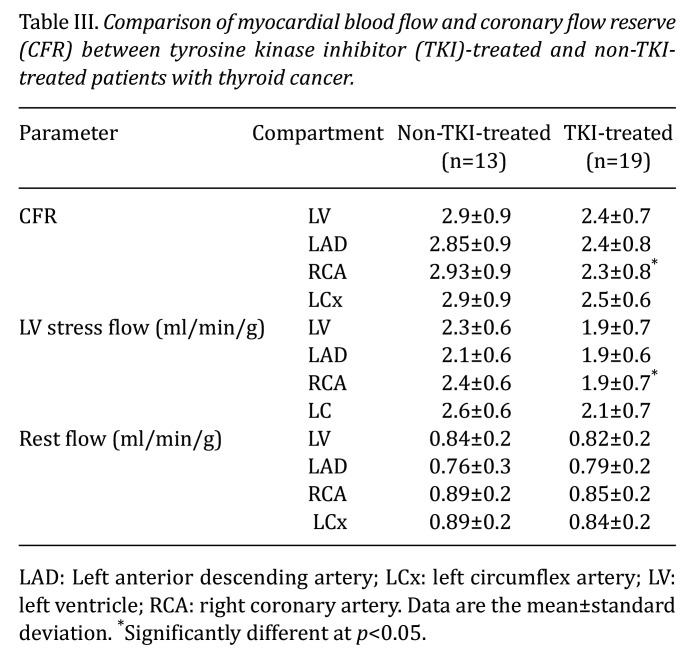
Results: qMPI indicated that the TKI-treated group (n=19) exhibited reduced MBF, CFR, and coronary flow capacity compared to the non-TKI-treated group. The right coronary artery (RCA) territory was notably affected by TKI treatment, particularly during the stress phase: RCA-stress blood flow: 2.4±0.6 vs. 1.9±0.7 ml/min/g; RCA-CFR: 2.3±0.8 vs. 2.93±0.9 for TKI-treated vs. non TKI-treated groups, respectively. This effect was more pronounced in the subgroup undergoing sequential anti-vascular endothelial growth factor TKI treatment (e.g. sorafenib and lenvatinib) (n=4) compared to non-TKI-treated controls. Additionally, TKI-treated patients showed a higher mean NT-ProBNP level (203±322.2 pg/ml) than non-TKI-treated patients (39.1±36 pg/ml). Abnormal MBF/CFR was also associated with higher cumulative RAIT dose and lower thyrotropin level.
Conclusion: TKI therapy, especially anti-vascular endothelial growth factor TKI, can negatively affect myocardial perfusion and lead to coronary microcirculation dysfunction, reducing MBF/CFR during the stress phase. The link between cumulative RAIT dose, lower thyroid-stimulating hormone level, and abnormal MBF/CFR highlights the need for further research.
期刊介绍:
IN VIVO is an international peer-reviewed journal designed to bring together original high quality works and reviews on experimental and clinical biomedical research within the frames of physiology, pathology and disease management.
The topics of IN VIVO include: 1. Experimental development and application of new diagnostic and therapeutic procedures; 2. Pharmacological and toxicological evaluation of new drugs, drug combinations and drug delivery systems; 3. Clinical trials; 4. Development and characterization of models of biomedical research; 5. Cancer diagnosis and treatment; 6. Immunotherapy and vaccines; 7. Radiotherapy, Imaging; 8. Tissue engineering, Regenerative medicine; 9. Carcinogenesis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


