Xinmin Duan, Xiaojing Song, Wei Lyu, Yanling Li, Jing Tang, Wei Cao, Yang Han, Taisheng Li
{"title":"HIV Low-Level Viremia is Not Related to Subsequent Virological Failure Under NNRTI-Based Regimens: A Multicenter Retrospective Study in China.","authors":"Xinmin Duan, Xiaojing Song, Wei Lyu, Yanling Li, Jing Tang, Wei Cao, Yang Han, Taisheng Li","doi":"10.2147/IDR.S533871","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The long-term impact of low-level viremia (LLV), defined as two consecutive viral loads (VL) of <200 copies/mL, on virological failure remains unclear. This study aimed to investigate the association between viremia patterns and virological failure in people living with HIV (PLWH) in China who predominantly received non-nucleoside reverse transcriptase inhibitor (NNRTI)-based therapies.</p><p><strong>Methods: </strong>Data from six HIV-infected cohorts in China were analyzed. Adult antiretroviral therapy (ART)-naïve patients were included. Patients were excluded if they received less than 24 weeks of ART, had fewer than two documented VL and CD4+ T cell count, initiated ART during the acute infection stage, or had a follow-up duration of less than 48 weeks. All patients were stratified according to virological suppression (VS), virological blips (VB), or LLV. Cox regression analysis was used to evaluate the association between virological failure and patterns of viremia. Genotypic drug resistance mutations were compared at baseline and during LLV.</p><p><strong>Results: </strong>Among the 1532 patients, 374 (24.4%) had blips and 166 (10.8%) had LLV. The LLV group had a higher baseline viral load and lower CD4<sup>+</sup> T cell count. Approximately 90% of patients received NNRTI-based regimens. In the adjusted Cox regression, neither the blip nor LLV groups demonstrated a significantly increased risk of virological failure compared to the VS group (Blip, adjusted HR = 0.5 [95% CI: 0.2-1.2], <i>p</i> = 0.116; LLV, aHR = 0.7 [95% CI: 0.3-1.9], <i>p</i> = 0.474). Among the 17 patients who successfully underwent sequencing, three (17.6%) developed new drug resistance mutations, but none experienced virological failure.</p><p><strong>Conclusion: </strong>Neither blip nor LLV were significantly associated with an increased risk of virological failure in China. Emerging drug resistance mutations in LLV are rare and do not correlate with subsequent virological failures. Further research is needed to understand the clinical significance of these patterns of viremia.</p>","PeriodicalId":13577,"journal":{"name":"Infection and Drug Resistance","volume":"18 ","pages":"4373-4384"},"PeriodicalIF":2.9000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399107/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infection and Drug Resistance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/IDR.S533871","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The long-term impact of low-level viremia (LLV), defined as two consecutive viral loads (VL) of <200 copies/mL, on virological failure remains unclear. This study aimed to investigate the association between viremia patterns and virological failure in people living with HIV (PLWH) in China who predominantly received non-nucleoside reverse transcriptase inhibitor (NNRTI)-based therapies.
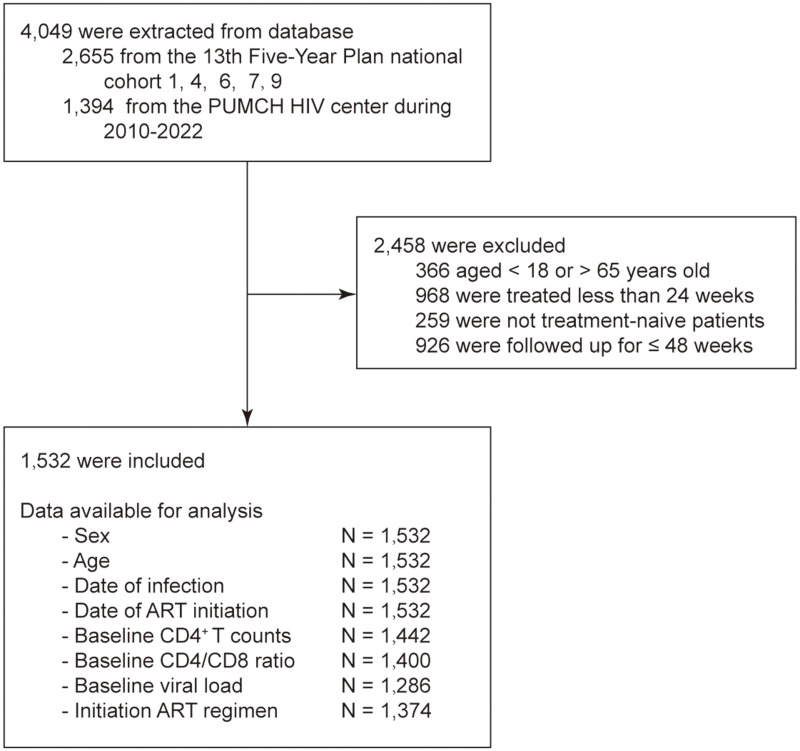
Methods: Data from six HIV-infected cohorts in China were analyzed. Adult antiretroviral therapy (ART)-naïve patients were included. Patients were excluded if they received less than 24 weeks of ART, had fewer than two documented VL and CD4+ T cell count, initiated ART during the acute infection stage, or had a follow-up duration of less than 48 weeks. All patients were stratified according to virological suppression (VS), virological blips (VB), or LLV. Cox regression analysis was used to evaluate the association between virological failure and patterns of viremia. Genotypic drug resistance mutations were compared at baseline and during LLV.
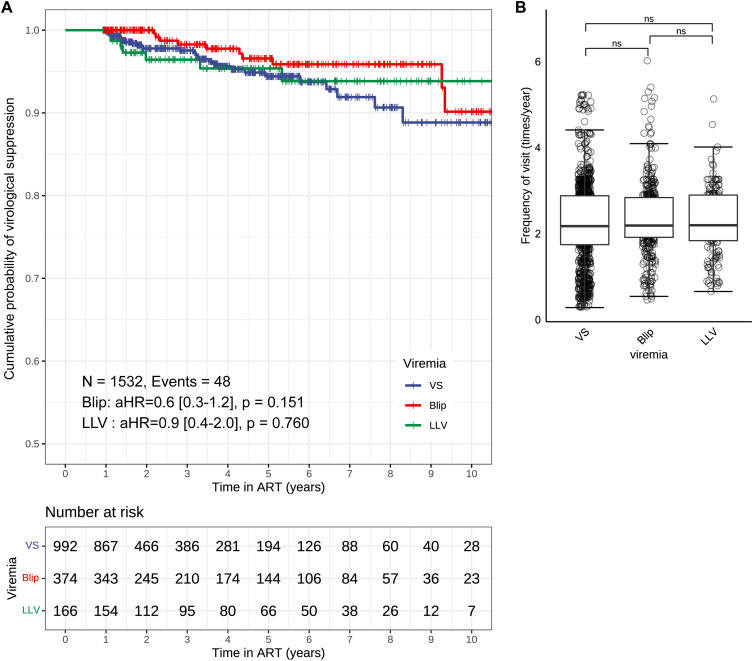
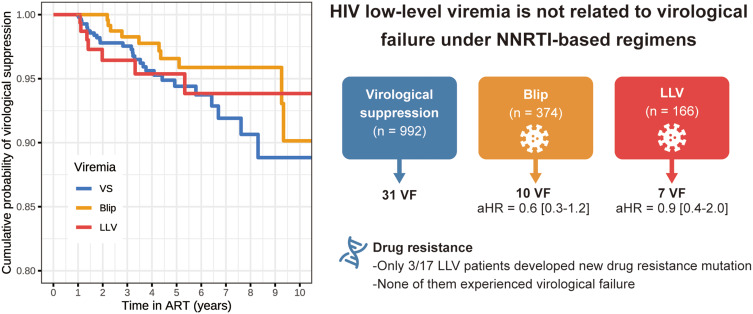
Results: Among the 1532 patients, 374 (24.4%) had blips and 166 (10.8%) had LLV. The LLV group had a higher baseline viral load and lower CD4+ T cell count. Approximately 90% of patients received NNRTI-based regimens. In the adjusted Cox regression, neither the blip nor LLV groups demonstrated a significantly increased risk of virological failure compared to the VS group (Blip, adjusted HR = 0.5 [95% CI: 0.2-1.2], p = 0.116; LLV, aHR = 0.7 [95% CI: 0.3-1.9], p = 0.474). Among the 17 patients who successfully underwent sequencing, three (17.6%) developed new drug resistance mutations, but none experienced virological failure.
Conclusion: Neither blip nor LLV were significantly associated with an increased risk of virological failure in China. Emerging drug resistance mutations in LLV are rare and do not correlate with subsequent virological failures. Further research is needed to understand the clinical significance of these patterns of viremia.
期刊介绍:
About Journal
Editors
Peer Reviewers
Articles
Article Publishing Charges
Aims and Scope
Call For Papers
ISSN: 1178-6973
Editor-in-Chief: Professor Suresh Antony
An international, peer-reviewed, open access journal that focuses on the optimal treatment of infection (bacterial, fungal and viral) and the development and institution of preventative strategies to minimize the development and spread of resistance.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


