From Screening to Strategy: Targeted Carbapenem-Resistant Enterobacteriaceae (CRE) Infection Prediction After Endoscopic Retrograde Cholangiopancreatography (ERCP).
Jundi Wang, Kaisheng Su, Shuying Wang, Yanfei Yang
{"title":"From Screening to Strategy: Targeted Carbapenem-Resistant Enterobacteriaceae (CRE) Infection Prediction After Endoscopic Retrograde Cholangiopancreatography (ERCP).","authors":"Jundi Wang, Kaisheng Su, Shuying Wang, Yanfei Yang","doi":"10.2147/IDR.S532928","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Invariably, patients can be exposed to Carbapenem-resistant Enterobacteriaceae (CRE) through contaminated device during Endoscopic retrograde cholangiopancreatography (ERCP). We aimed to identify the risk factors and establish a model for predicting subsequent CRE infections in patients with CRE-positive bile screening after ERCP.</p><p><strong>Methods: </strong>Patients underwent ERCP were performed with bile active screening of CRE. Medical records were reviewed to identify patient demographics, comorbidities, microbiology and antimicrobial treatments. The results were grouped according to the occurrence of subsequent CRE infection, and the patients were divided into two groups: a CRE infection group and a non-CRE infection group. The diagnosis for CRE infection was confirmed by more than 2 physicians. Logistic regression methods were used to determine the risk factors for CRE infections. The risk prediction model was constructed by integrating the clinical data and the result of logistic regression, by a nomogram and forest plot. Finally, goodness of fit of the final model was tested using the likelihood ratio test.</p><p><strong>Results: </strong>Central venous catheterization (OR=11.32; 95% CI 1.15-40.62), cholecystitis (OR=3.82; 95% CI 1.12-13.01), malignancy (OR=4.33; 95% CI 1.41-13.35) and the antimicrobial drug use (OR=1.08; 95% CI 1.03-1.14) were considered as highly relevant risk factors for subsequent CRE infections in bile active screening positive patients. The goodness of fit test indicated that the model was well-calibrated for both groups.</p><p><strong>Conclusion: </strong>A targeted active screening in bile samples can be beneficial for patients with high risk factors of CRE infections. The nomogram developed in this study can help clinicians accurately predict the possibility of patients with subsequent CRE infections after ERCP, so as to facilitate more precise individualized treatment.</p>","PeriodicalId":13577,"journal":{"name":"Infection and Drug Resistance","volume":"18 ","pages":"4189-4199"},"PeriodicalIF":2.9000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12375330/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infection and Drug Resistance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/IDR.S532928","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Invariably, patients can be exposed to Carbapenem-resistant Enterobacteriaceae (CRE) through contaminated device during Endoscopic retrograde cholangiopancreatography (ERCP). We aimed to identify the risk factors and establish a model for predicting subsequent CRE infections in patients with CRE-positive bile screening after ERCP.
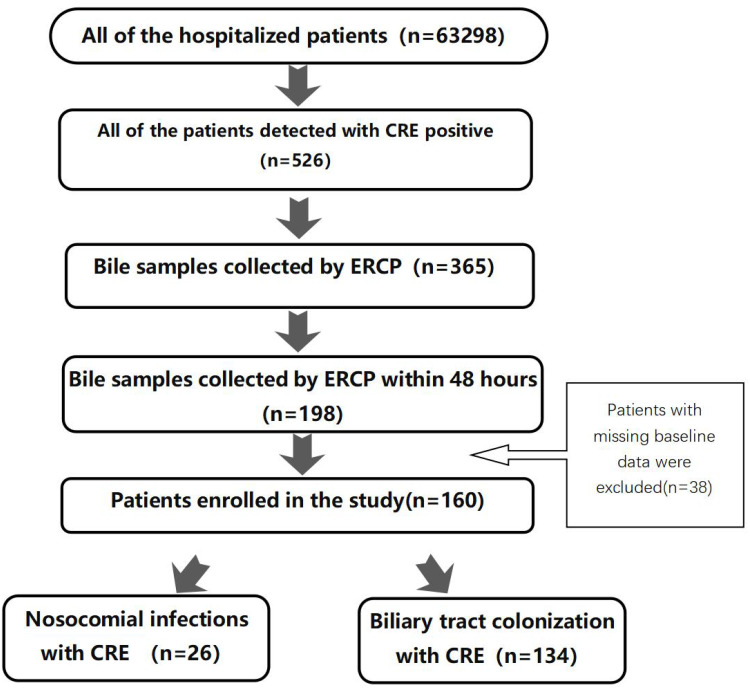
Methods: Patients underwent ERCP were performed with bile active screening of CRE. Medical records were reviewed to identify patient demographics, comorbidities, microbiology and antimicrobial treatments. The results were grouped according to the occurrence of subsequent CRE infection, and the patients were divided into two groups: a CRE infection group and a non-CRE infection group. The diagnosis for CRE infection was confirmed by more than 2 physicians. Logistic regression methods were used to determine the risk factors for CRE infections. The risk prediction model was constructed by integrating the clinical data and the result of logistic regression, by a nomogram and forest plot. Finally, goodness of fit of the final model was tested using the likelihood ratio test.
Results: Central venous catheterization (OR=11.32; 95% CI 1.15-40.62), cholecystitis (OR=3.82; 95% CI 1.12-13.01), malignancy (OR=4.33; 95% CI 1.41-13.35) and the antimicrobial drug use (OR=1.08; 95% CI 1.03-1.14) were considered as highly relevant risk factors for subsequent CRE infections in bile active screening positive patients. The goodness of fit test indicated that the model was well-calibrated for both groups.
Conclusion: A targeted active screening in bile samples can be beneficial for patients with high risk factors of CRE infections. The nomogram developed in this study can help clinicians accurately predict the possibility of patients with subsequent CRE infections after ERCP, so as to facilitate more precise individualized treatment.
背景:在内镜逆行胰胆管造影(ERCP)中,患者不可避免地会通过污染的设备暴露于耐碳青霉烯类肠杆菌科(CRE)。我们的目的是确定危险因素,并建立预测ERCP后CRE阳性胆汁筛查患者后续CRE感染的模型。方法:对ERCP患者行CRE胆汁活性筛查。对医疗记录进行了审查,以确定患者人口统计、合并症、微生物学和抗菌治疗。根据后续CRE感染的发生情况对结果进行分组,将患者分为CRE感染组和非CRE感染组。CRE感染的诊断经2名以上医生确认。采用Logistic回归方法确定CRE感染的危险因素。综合临床资料和logistic回归结果,采用nomogram和forest plot,构建风险预测模型。最后,采用似然比检验对最终模型的拟合优度进行检验。结果:中心静脉置管(OR=11.32; 95% CI 1.15-40.62)、胆囊炎(OR=3.82; 95% CI 1.12-13.01)、恶性肿瘤(OR=4.33; 95% CI 1.41-13.35)和抗菌药物使用(OR=1.08; 95% CI 1.03-1.14)被认为是胆汁主动筛查阳性患者随后发生CRE感染的高度相关危险因素。拟合优度检验表明,该模型对两组均校正良好。结论:胆汁样本有针对性的主动筛查对CRE感染高危因素患者有益。本研究建立的nomogram影像图可以帮助临床医生准确预测ERCP术后患者发生CRE感染的可能性,从而更加精准的进行个体化治疗。
期刊介绍:
About Journal
Editors
Peer Reviewers
Articles
Article Publishing Charges
Aims and Scope
Call For Papers
ISSN: 1178-6973
Editor-in-Chief: Professor Suresh Antony
An international, peer-reviewed, open access journal that focuses on the optimal treatment of infection (bacterial, fungal and viral) and the development and institution of preventative strategies to minimize the development and spread of resistance.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


