{"title":"Robotic <i>Versus</i> Laparoscopic Pelvic Lymphadenectomy for Endometrial Cancer Under the Japanese Public Health Insurance System.","authors":"Hikaru Imatake, Kana Kawai, Yuka Matsumoto, Yuri Suminaga, Chihiro Nakai, Yuriko Tanabe, Naoya Kishimoto, Ikuko Emoto, Yasuaki Amano, Kaoru Abiko","doi":"10.21873/invivo.14078","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Surgery is the preferred treatment modality for endometrial cancer. In recent years, minimally invasive surgery (MIS) has become increasingly popular, and in Japan, robotic surgery has been covered by national insurance in addition to laparoscopic surgery for apparent stage IA cases since 2018. We conducted a comparative analysis of laparoscopic and robotic surgeries, including pelvic lymphadenectomy for stage IA endometrial cancer, with the aim of evaluating the efficacy of robotic surgery.</p><p><strong>Patients and methods: </strong>A retrospective analysis was conducted for patients who underwent MIS pelvic lymphadenectomy between January 2018 and December 2023. Sixty-nine patients who underwent robotic surgery and 29 who underwent laparoscopic surgery were included in the study. All the patients underwent total hysterectomy and pelvic lymph node dissection, with preoperative diagnosis of stage 1A and G1-G2 endometrial cancer.</p><p><strong>Results: </strong>Operative time was longer in the robotic group (median=316 <i>vs.</i> 272 min in the laparoscopic group, <i>p</i>=0.02). Intraoperative blood loss and postoperative hospital stay were lower in the robotic group (median blood loss: 0 <i>vs.</i> 50 ml for the laparoscopic group, <i>p</i><0.01; median postoperative hospital stay: 5 <i>vs.</i> 8 days for the laparoscopic group, <i>p</i><0.01). No statistically significant differences were found in the incidence of complications and recurrence between the two groups.</p><p><strong>Conclusion: </strong>This retrospective analysis suggests that robotic surgery is a feasible and safe procedure for total hysterectomy and pelvic lymph node dissection in patients with preoperative diagnosis of stage IA and G1-G2 endometrial cancer.</p>","PeriodicalId":13364,"journal":{"name":"In vivo","volume":"39 5","pages":"2794-2800"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396043/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"In vivo","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21873/invivo.14078","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aim: Surgery is the preferred treatment modality for endometrial cancer. In recent years, minimally invasive surgery (MIS) has become increasingly popular, and in Japan, robotic surgery has been covered by national insurance in addition to laparoscopic surgery for apparent stage IA cases since 2018. We conducted a comparative analysis of laparoscopic and robotic surgeries, including pelvic lymphadenectomy for stage IA endometrial cancer, with the aim of evaluating the efficacy of robotic surgery.
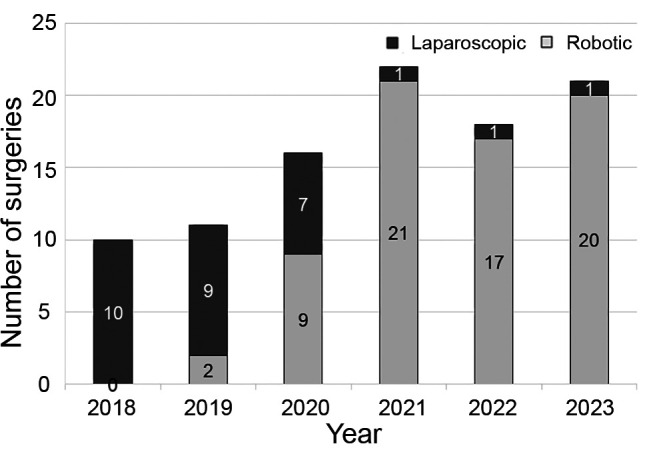
Patients and methods: A retrospective analysis was conducted for patients who underwent MIS pelvic lymphadenectomy between January 2018 and December 2023. Sixty-nine patients who underwent robotic surgery and 29 who underwent laparoscopic surgery were included in the study. All the patients underwent total hysterectomy and pelvic lymph node dissection, with preoperative diagnosis of stage 1A and G1-G2 endometrial cancer.
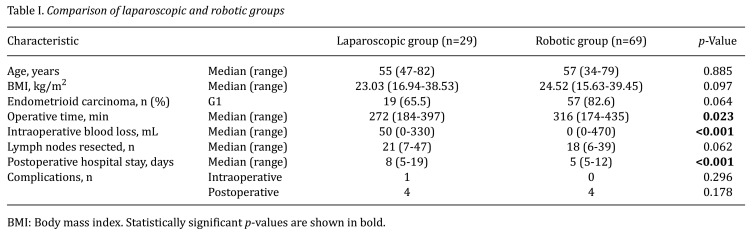
Results: Operative time was longer in the robotic group (median=316 vs. 272 min in the laparoscopic group, p=0.02). Intraoperative blood loss and postoperative hospital stay were lower in the robotic group (median blood loss: 0 vs. 50 ml for the laparoscopic group, p<0.01; median postoperative hospital stay: 5 vs. 8 days for the laparoscopic group, p<0.01). No statistically significant differences were found in the incidence of complications and recurrence between the two groups.
Conclusion: This retrospective analysis suggests that robotic surgery is a feasible and safe procedure for total hysterectomy and pelvic lymph node dissection in patients with preoperative diagnosis of stage IA and G1-G2 endometrial cancer.
背景/目的:手术是子宫内膜癌的首选治疗方式。近年来,微创手术(MIS)越来越受欢迎,在日本,自2018年以来,除了对明显的IA期病例进行腹腔镜手术外,机器人手术已被纳入国民保险。我们对腹腔镜和机器人手术进行了比较分析,包括盆腔淋巴结切除术治疗IA期子宫内膜癌,目的是评估机器人手术的疗效。患者和方法:对2018年1月至2023年12月期间接受MIS盆腔淋巴结切除术的患者进行回顾性分析。69名接受机器人手术的患者和29名接受腹腔镜手术的患者参与了这项研究。所有患者均行全子宫切除术和盆腔淋巴结清扫术,术前诊断为1A期和G1-G2期子宫内膜癌。结果:机器人组手术时间更长(中位数为316分钟,腹腔镜组为272分钟,p=0.02)。机器人组术中出血量和术后住院时间较低(中位出血量:0 ml vs.腹腔镜组50 ml, pvs)。结论:本回顾性分析提示,对于术前诊断为IA期和G1-G2期子宫内膜癌的患者,机器人手术是一种可行且安全的全子宫切除和盆腔淋巴结清扫手术。
期刊介绍:
IN VIVO is an international peer-reviewed journal designed to bring together original high quality works and reviews on experimental and clinical biomedical research within the frames of physiology, pathology and disease management.
The topics of IN VIVO include: 1. Experimental development and application of new diagnostic and therapeutic procedures; 2. Pharmacological and toxicological evaluation of new drugs, drug combinations and drug delivery systems; 3. Clinical trials; 4. Development and characterization of models of biomedical research; 5. Cancer diagnosis and treatment; 6. Immunotherapy and vaccines; 7. Radiotherapy, Imaging; 8. Tissue engineering, Regenerative medicine; 9. Carcinogenesis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


