The risk of hepatocellular carcinoma recurrence after liver transplantation increases with locoregional therapies in patients initially within Milan criteria.
Jinsoo Rhu, Namkee Oh, Gyu-Seong Choi, Jongman Kim, Jae-Won Joh
{"title":"The risk of hepatocellular carcinoma recurrence after liver transplantation increases with locoregional therapies in patients initially within Milan criteria.","authors":"Jinsoo Rhu, Namkee Oh, Gyu-Seong Choi, Jongman Kim, Jae-Won Joh","doi":"10.21037/hbsn-24-107","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal timing of transplantation for hepatocellular carcinoma (HCC) is still under debate regarding the tumor biology and locoregional control with various treatments. We designed this study to find out what kind of factors affect the post-transplantation outcome focusing on the timing of transplantation.</p><p><strong>Methods: </strong>We analyzed HCC patients who met the Milan criteria at the initial stage and subsequently underwent liver transplantation (LT) between 2007 and 2020. We examined the number of locoregional therapies (LRTs) received, as well as data on tumor recurrence and survival. The number of LRTs was categorized into four groups: none, one or two, three or four, and five or more. Both recurrence-free survival and overall survival were analyzed.</p><p><strong>Results: </strong>A total of 423 patients who met the Milan criteria at the initial stage underwent LT. The median number of LRTs before transplantation was 2, with an interquartile range of 0 to 4. There were 112 patients (26.5%) who underwent LT as the initial treatment. Multivariable Cox analyses showed that the number of LRTs [hazard ratio (HR) =1.219, 95% confidence interval (CI): 1.074-1.382, P=0.002] was a significant factor for recurrence. When analyzed as a categorical variable, three or four LRTs (HR =4.936, 95% CI: 1.790-13.615, P=0.002) and five or more LRTs (HR =5.129, 95% CI: 1.958-13.440, P=0.001) showed a significantly higher risk compared to the primary transplantation group.<b>Conclusions:</b> This study showed that the risk of recurrence after transplantation increases with the increasing number of LRTs prior to LT. Therefore, optimal timing of LT should be cautiously decided in regards of recurrence potential of each patient.</p>","PeriodicalId":12878,"journal":{"name":"Hepatobiliary surgery and nutrition","volume":"14 4","pages":"539-551"},"PeriodicalIF":7.8000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12393127/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatobiliary surgery and nutrition","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/hbsn-24-107","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/5 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The optimal timing of transplantation for hepatocellular carcinoma (HCC) is still under debate regarding the tumor biology and locoregional control with various treatments. We designed this study to find out what kind of factors affect the post-transplantation outcome focusing on the timing of transplantation.
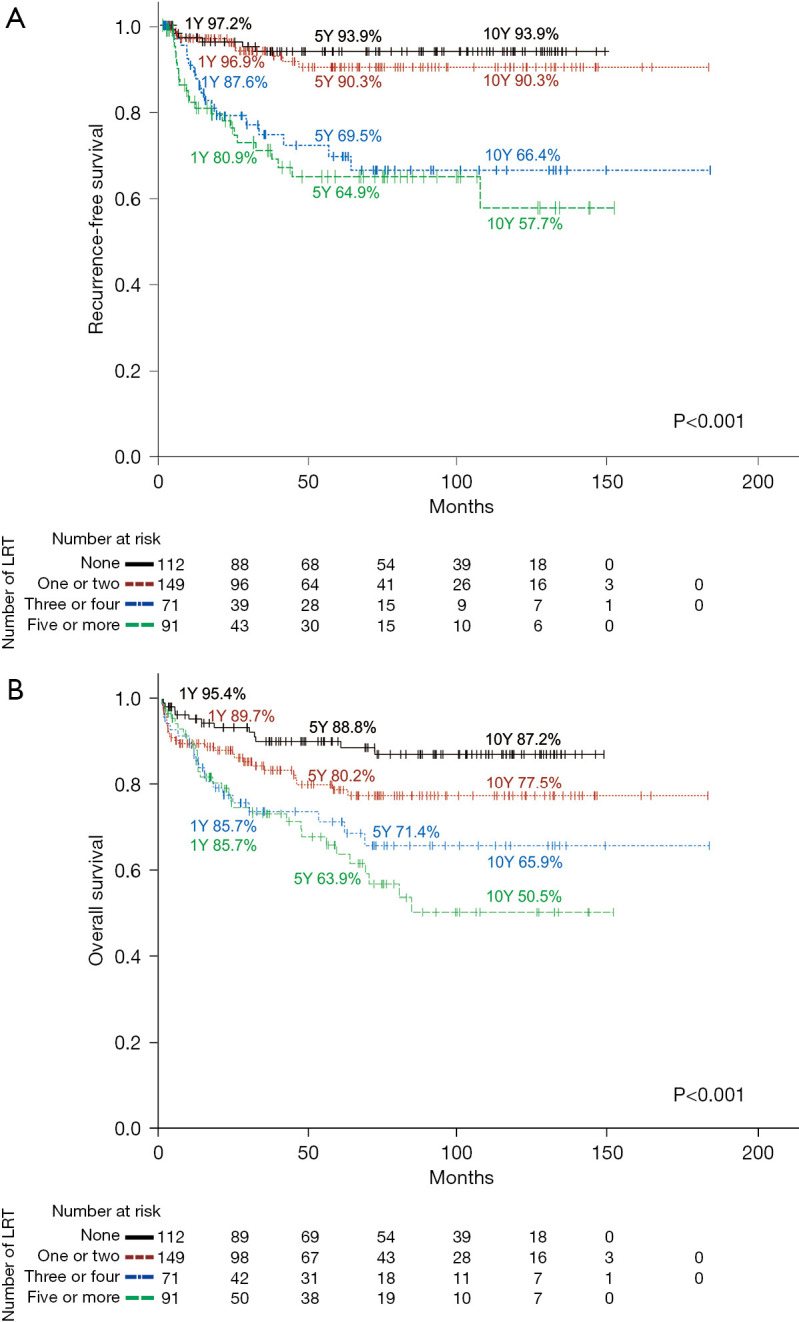
Methods: We analyzed HCC patients who met the Milan criteria at the initial stage and subsequently underwent liver transplantation (LT) between 2007 and 2020. We examined the number of locoregional therapies (LRTs) received, as well as data on tumor recurrence and survival. The number of LRTs was categorized into four groups: none, one or two, three or four, and five or more. Both recurrence-free survival and overall survival were analyzed.
Results: A total of 423 patients who met the Milan criteria at the initial stage underwent LT. The median number of LRTs before transplantation was 2, with an interquartile range of 0 to 4. There were 112 patients (26.5%) who underwent LT as the initial treatment. Multivariable Cox analyses showed that the number of LRTs [hazard ratio (HR) =1.219, 95% confidence interval (CI): 1.074-1.382, P=0.002] was a significant factor for recurrence. When analyzed as a categorical variable, three or four LRTs (HR =4.936, 95% CI: 1.790-13.615, P=0.002) and five or more LRTs (HR =5.129, 95% CI: 1.958-13.440, P=0.001) showed a significantly higher risk compared to the primary transplantation group.Conclusions: This study showed that the risk of recurrence after transplantation increases with the increasing number of LRTs prior to LT. Therefore, optimal timing of LT should be cautiously decided in regards of recurrence potential of each patient.
期刊介绍:
Hepatobiliary Surgery and Nutrition (HBSN) is a bi-monthly, open-access, peer-reviewed journal (Print ISSN: 2304-3881; Online ISSN: 2304-389X) since December 2012. The journal focuses on hepatopancreatobiliary disease and nutrition, aiming to present new findings and deliver up-to-date, practical information on diagnosis, prevention, and clinical investigations. Areas of interest cover surgical techniques, clinical and basic research, transplantation, therapies, NASH, NAFLD, targeted drugs, gut microbiota, metabolism, cancer immunity, genomics, and nutrition and dietetics. HBSN serves as a valuable resource for professionals seeking insights into diverse aspects of hepatobiliary surgery and nutrition.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


