Matthew Jarocki, Sophie Green, Henry H L Wu, Rajkumar Chinnadurai
{"title":"Cardiorenal Syndrome in the Elderly: Challenges and Considerations.","authors":"Matthew Jarocki, Sophie Green, Henry H L Wu, Rajkumar Chinnadurai","doi":"10.3390/geriatrics10040104","DOIUrl":null,"url":null,"abstract":"<p><p>Cardiorenal syndrome (CRS) is a term used to describe the combined dysfunction of the heart and kidneys. This complex disorder is widely acknowledged to be challenging in both its diagnosis and management, and this is the case particularly in the elderly population, due to multi-morbidity, polypharmacy, and age-related physiological changes. Given advancements in medicine and more prolonged cumulative exposure to risk factors in the elderly population, it is likely that the prevalence of chronic kidney disease (CKD) and heart failure (HF) will continue to rise going forward. Hence, understanding the mechanisms involved in the development of CRS is paramount. There are five different CRS types-they are categorised depending on the primary organ involved the acuity of disease. The pathophysiological process behind CRS is complex, involving the interplay of many processes including hemodynamic changes, neurohormonal activation, inflammation, oxidative stress, and endothelial dysfunction and vascular stiffness. The numerous diagnostic and management challenges associated with CRS are significantly further exacerbated in an elderly population. Biomarkers used to aid the diagnosis of CRS, such as serum creatinine and brain natriuretic peptide (BNP), can be challenging to interpret in the elderly population due to age-related renal senescence and multiple comorbidities. Polypharmacy can contribute to the development of CRS and therefore, before initiating treatment, coordinating a patient-centred, multi-speciality, holistic review to assess potential risks versus benefits of prescribed treatments is crucial. The overall prognosis of CRS in the elderly remains poor. Treatments are primarily directed at addressing the sequelae of the underlying aetiology, which often involves the removal of fluid through diuretics or ultrafiltration. Careful considerations when managing elderly patients with CRS is essential due to the high prevalence of frailty and functional decline. As such, in these patients, early discussions around advance care planning should be prioritised.</p>","PeriodicalId":12653,"journal":{"name":"Geriatrics","volume":"10 4","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12385558/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geriatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/geriatrics10040104","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
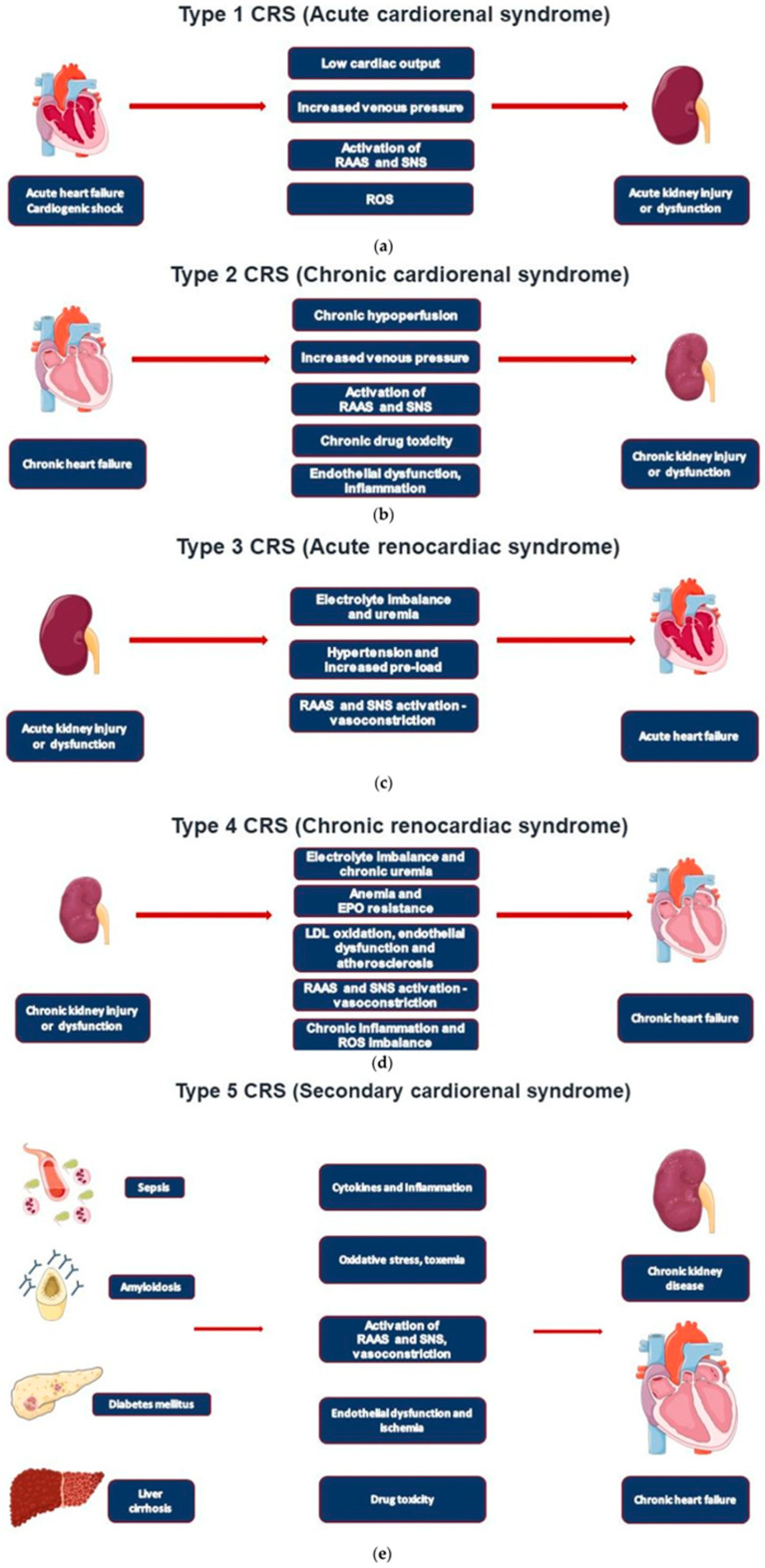
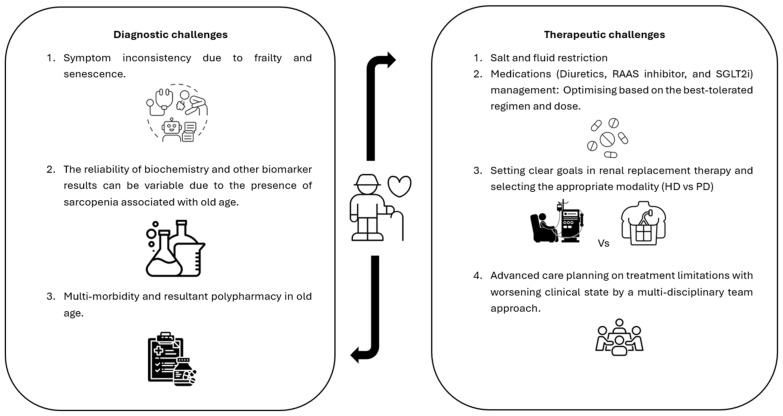
Cardiorenal syndrome (CRS) is a term used to describe the combined dysfunction of the heart and kidneys. This complex disorder is widely acknowledged to be challenging in both its diagnosis and management, and this is the case particularly in the elderly population, due to multi-morbidity, polypharmacy, and age-related physiological changes. Given advancements in medicine and more prolonged cumulative exposure to risk factors in the elderly population, it is likely that the prevalence of chronic kidney disease (CKD) and heart failure (HF) will continue to rise going forward. Hence, understanding the mechanisms involved in the development of CRS is paramount. There are five different CRS types-they are categorised depending on the primary organ involved the acuity of disease. The pathophysiological process behind CRS is complex, involving the interplay of many processes including hemodynamic changes, neurohormonal activation, inflammation, oxidative stress, and endothelial dysfunction and vascular stiffness. The numerous diagnostic and management challenges associated with CRS are significantly further exacerbated in an elderly population. Biomarkers used to aid the diagnosis of CRS, such as serum creatinine and brain natriuretic peptide (BNP), can be challenging to interpret in the elderly population due to age-related renal senescence and multiple comorbidities. Polypharmacy can contribute to the development of CRS and therefore, before initiating treatment, coordinating a patient-centred, multi-speciality, holistic review to assess potential risks versus benefits of prescribed treatments is crucial. The overall prognosis of CRS in the elderly remains poor. Treatments are primarily directed at addressing the sequelae of the underlying aetiology, which often involves the removal of fluid through diuretics or ultrafiltration. Careful considerations when managing elderly patients with CRS is essential due to the high prevalence of frailty and functional decline. As such, in these patients, early discussions around advance care planning should be prioritised.
期刊介绍:
• Geriatric biology
• Geriatric health services research
• Geriatric medicine research
• Geriatric neurology, stroke, cognition and oncology
• Geriatric surgery
• Geriatric physical functioning, physical health and activity
• Geriatric psychiatry and psychology
• Geriatric nutrition
• Geriatric epidemiology
• Geriatric rehabilitation

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


