Liping Wang, Eveline P van Poelgeest, Marjolein Klop, Jurgen A H R Claassen, Alfons G Hoekstra, Nathalie van der Velde
{"title":"Beat-to-Beat Blood Pressure Monitoring and Orthostatic Hypotension-Related Falls in Two Cohorts of Older Adults.","authors":"Liping Wang, Eveline P van Poelgeest, Marjolein Klop, Jurgen A H R Claassen, Alfons G Hoekstra, Nathalie van der Velde","doi":"10.3390/geriatrics10040102","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Falls are a major public health issue among older adults, often related to postural or orthostatic hypotension (OH). The optimal timing and methods for measuring blood pressure (BP) to assess OH and its relationship with falls are uncertain. <b>Methods:</b> We analyzed data from two older cohorts: the PROHEALTH study (<i>n</i> = 30, aged ≥ 65 years) and the NILVAD-CBF trial (<i>n</i> = 58, aged ≥ 50 years). Continuous beat-to-beat BP was measured during active stand tests. We assessed orthostatic BP responses during sit-to-stand and supine-to-stand maneuvers and calculated the associations between orthostatic BP response variables and falls. <b>Results:</b> In the PROHEALTH cohort, participants with a history of falls exhibited a significantly lower baseline BP (115 ± 13/68 ± 10 vs. 142 ± 21/79 ± 11 mmHg; <i>p</i> = 0.004/0.018) and lower systolic BP (SBP) nadir (90 ± 22 vs. 112 ± 25 mmHg; <i>p</i> = 0.043) than non-fallers. SBP recovery within three minutes post-stand was delayed in fallers but rapid in non-fallers. A lower resting BP was associated with fall risk, and a lower BP nadir within 10 s after standing showed a trend toward a higher fall risk. No significant associations were found in the NILVAD-CBF cohort (prospective falls). <b>Conclusions:</b> Our findings demonstrate that a lower resting SBP and diastolic BP (DBP) are associated with an increased fall risk in older adults, with a lower SBP and DBP nadir after standing also showing a potential association. Persistent OH or delayed BP recovery is identified as a potentially relevant fall risk factor. The supine-to-stand test was more sensitive in detecting OH than the sit-to-stand test. Continuous BP monitoring provides the advantage of detecting pathophysiologic orthostatic BP responses for fall risk assessment in older adults. Further research with larger cohorts is warranted to validate our findings.</p>","PeriodicalId":12653,"journal":{"name":"Geriatrics","volume":"10 4","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12385785/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geriatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/geriatrics10040102","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
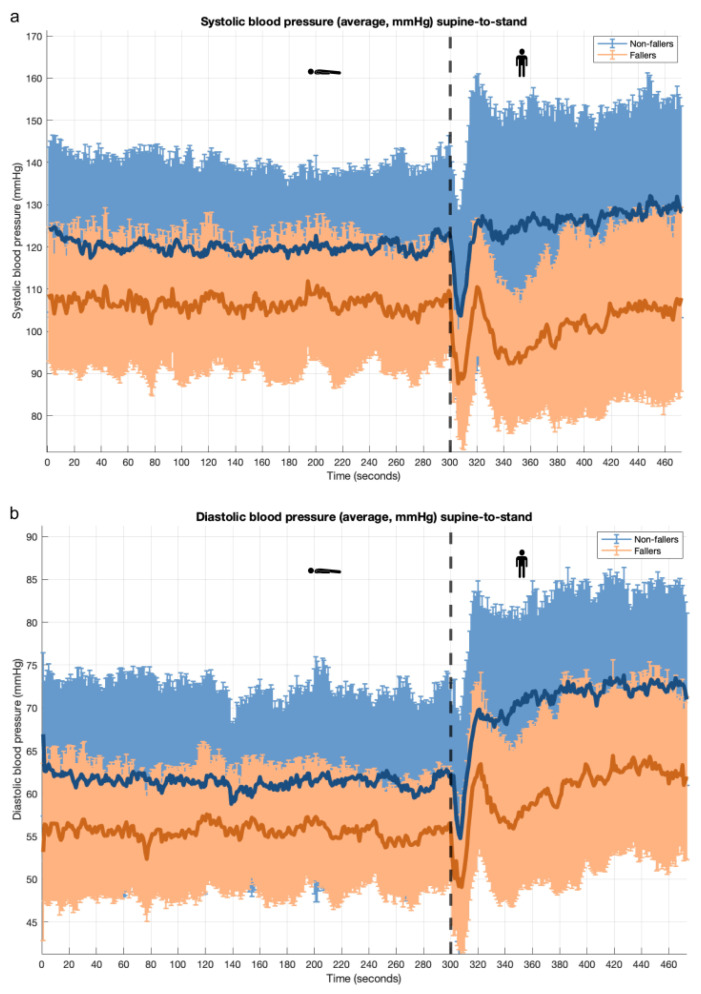
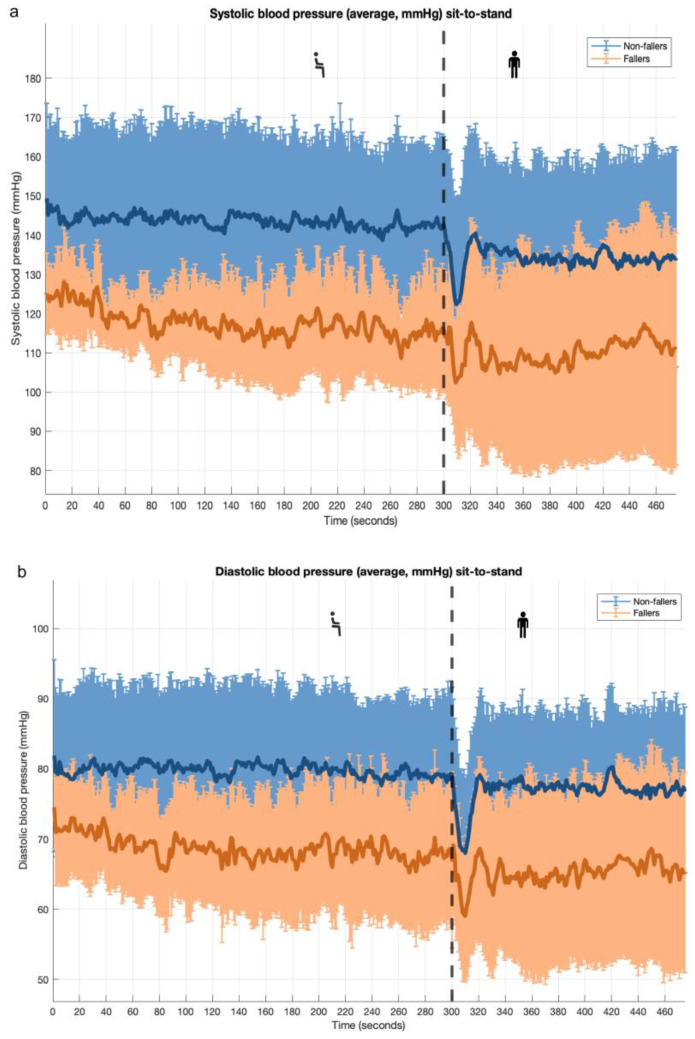
Background: Falls are a major public health issue among older adults, often related to postural or orthostatic hypotension (OH). The optimal timing and methods for measuring blood pressure (BP) to assess OH and its relationship with falls are uncertain. Methods: We analyzed data from two older cohorts: the PROHEALTH study (n = 30, aged ≥ 65 years) and the NILVAD-CBF trial (n = 58, aged ≥ 50 years). Continuous beat-to-beat BP was measured during active stand tests. We assessed orthostatic BP responses during sit-to-stand and supine-to-stand maneuvers and calculated the associations between orthostatic BP response variables and falls. Results: In the PROHEALTH cohort, participants with a history of falls exhibited a significantly lower baseline BP (115 ± 13/68 ± 10 vs. 142 ± 21/79 ± 11 mmHg; p = 0.004/0.018) and lower systolic BP (SBP) nadir (90 ± 22 vs. 112 ± 25 mmHg; p = 0.043) than non-fallers. SBP recovery within three minutes post-stand was delayed in fallers but rapid in non-fallers. A lower resting BP was associated with fall risk, and a lower BP nadir within 10 s after standing showed a trend toward a higher fall risk. No significant associations were found in the NILVAD-CBF cohort (prospective falls). Conclusions: Our findings demonstrate that a lower resting SBP and diastolic BP (DBP) are associated with an increased fall risk in older adults, with a lower SBP and DBP nadir after standing also showing a potential association. Persistent OH or delayed BP recovery is identified as a potentially relevant fall risk factor. The supine-to-stand test was more sensitive in detecting OH than the sit-to-stand test. Continuous BP monitoring provides the advantage of detecting pathophysiologic orthostatic BP responses for fall risk assessment in older adults. Further research with larger cohorts is warranted to validate our findings.
期刊介绍:
• Geriatric biology
• Geriatric health services research
• Geriatric medicine research
• Geriatric neurology, stroke, cognition and oncology
• Geriatric surgery
• Geriatric physical functioning, physical health and activity
• Geriatric psychiatry and psychology
• Geriatric nutrition
• Geriatric epidemiology
• Geriatric rehabilitation

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


