Kush Mody, Avani A Chopra, David Ahn, Michael Aynardi, Sheldon Lin
{"title":"Cost-Effectiveness Thresholds for Venous Thromboembolism Prophylaxis in Ankle Fracture Surgery: A Break-Even Analysis.","authors":"Kush Mody, Avani A Chopra, David Ahn, Michael Aynardi, Sheldon Lin","doi":"10.1177/24730114251363497","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of venous thromboembolism (VTE) chemoprophylaxis following ankle fracture surgery remains controversial. Although pharmacologic prophylaxis is standard in major orthopaedic procedures, its utility in foot and ankle trauma surgery is unclear because of low reported VTE rates and potential bleeding risks. Furthermore, no consensus exists on the cost-effectiveness of prophylactic agents in this population.</p><p><strong>Methods: </strong>A literature review and the TriNetX Research Network were used to identify postoperative symptomatic VTE rates following ankle open reduction internal fixation (ORIF). The cost of treating a symptomatic VTE was estimated from existing literature and adjusted to 2025 US dollars. Drug pricing data were obtained from an online pharmacy database. A break-even analysis was conducted to calculate the absolute risk reduction (ARR) and number needed to treat (NNT) for each agent to be cost-effective. A subanalysis compared 30-day bleeding and transfusion rates between patients who received prophylaxis and those who did not.</p><p><strong>Results: </strong>The low and high literature-based VTE rates were 0.33% and 1.2%, whereas the TriNetX-derived VTE rate was 0.56%. Among 64 184 patients undergoing ankle ORIF without prophylaxis, 384 developed a symptomatic VTE. Aspirin (81 mg and 325 mg) and warfarin (5 mg) were cost-effective at all 3 VTE rates, with NNTs ranging from 9217 to 10 547. Enoxaparin (40 mg) was only cost-effective at the highest VTE rate (NNT = 131), whereas rivaroxaban (20 mg) was not cost-effective at any rate. Enoxaparin and rivaroxaban became cost-effective only when VTE treatment costs exceeded $50 000 and $1 500 000, respectively. Patients receiving prophylaxis had higher bleeding (0.56% vs 0.26%) and transfusion (0.82% vs 0.25%) rates (<i>P</i> < .001).</p><p><strong>Conclusion: </strong>In summary, this study found that aspirin 81 mg, aspirin 325 mg, and warfarin are cost-effective for VTE chemoprophylaxis following ankle fracture fixation. Enoxaparin and rivaroxaban are generally not cost-effective, and their use may be appropriate only in high-risk patients.</p><p><strong>Level of evidence: </strong>Level IV, economic analysis.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"10 3","pages":"24730114251363497"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12368401/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114251363497","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The role of venous thromboembolism (VTE) chemoprophylaxis following ankle fracture surgery remains controversial. Although pharmacologic prophylaxis is standard in major orthopaedic procedures, its utility in foot and ankle trauma surgery is unclear because of low reported VTE rates and potential bleeding risks. Furthermore, no consensus exists on the cost-effectiveness of prophylactic agents in this population.
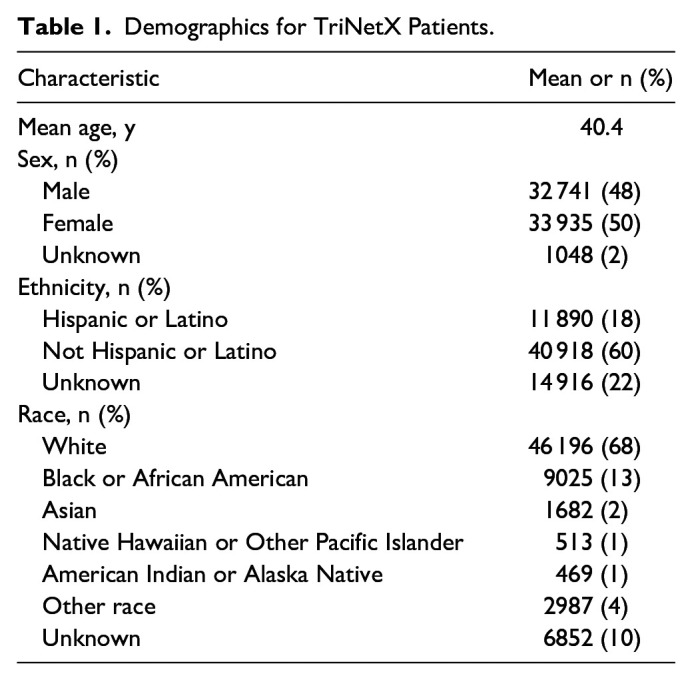
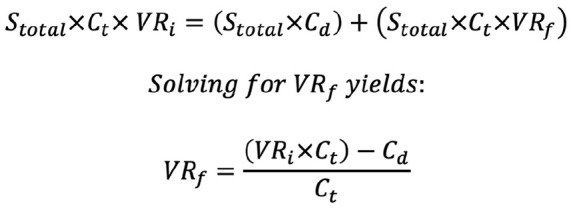
Methods: A literature review and the TriNetX Research Network were used to identify postoperative symptomatic VTE rates following ankle open reduction internal fixation (ORIF). The cost of treating a symptomatic VTE was estimated from existing literature and adjusted to 2025 US dollars. Drug pricing data were obtained from an online pharmacy database. A break-even analysis was conducted to calculate the absolute risk reduction (ARR) and number needed to treat (NNT) for each agent to be cost-effective. A subanalysis compared 30-day bleeding and transfusion rates between patients who received prophylaxis and those who did not.
Results: The low and high literature-based VTE rates were 0.33% and 1.2%, whereas the TriNetX-derived VTE rate was 0.56%. Among 64 184 patients undergoing ankle ORIF without prophylaxis, 384 developed a symptomatic VTE. Aspirin (81 mg and 325 mg) and warfarin (5 mg) were cost-effective at all 3 VTE rates, with NNTs ranging from 9217 to 10 547. Enoxaparin (40 mg) was only cost-effective at the highest VTE rate (NNT = 131), whereas rivaroxaban (20 mg) was not cost-effective at any rate. Enoxaparin and rivaroxaban became cost-effective only when VTE treatment costs exceeded $50 000 and $1 500 000, respectively. Patients receiving prophylaxis had higher bleeding (0.56% vs 0.26%) and transfusion (0.82% vs 0.25%) rates (P < .001).
Conclusion: In summary, this study found that aspirin 81 mg, aspirin 325 mg, and warfarin are cost-effective for VTE chemoprophylaxis following ankle fracture fixation. Enoxaparin and rivaroxaban are generally not cost-effective, and their use may be appropriate only in high-risk patients.
背景:踝关节骨折术后静脉血栓栓塞(VTE)化学预防的作用仍然存在争议。虽然药物预防在主要骨科手术中是标准的,但由于静脉血栓栓塞发生率低和潜在出血风险,其在足部和踝关节创伤手术中的应用尚不清楚。此外,在这一人群中,预防药物的成本效益尚未达成共识。方法:通过文献回顾和TriNetX研究网络来确定踝关节切开复位内固定(ORIF)术后症状性静脉血栓栓塞率。治疗症状性静脉血栓栓塞的费用是根据现有文献估计的,并调整为2025美元。药品定价数据来自在线药房数据库。进行盈亏平衡分析,以计算每种药物的绝对风险降低(ARR)和需要治疗的数量(NNT)以达到成本效益。一项亚分析比较了接受预防治疗和未接受预防治疗的患者30天出血和输血率。结果:基于文献的低、高VTE率分别为0.33%和1.2%,而trinetx衍生的VTE率为0.56%。在64 184例未进行预防的踝关节ORIF患者中,384例出现症状性静脉血栓栓塞。阿司匹林(81毫克和325毫克)和华法林(5毫克)在所有3种静脉血栓栓塞率下都具有成本效益,nnt范围从9217到10547。依诺肝素(40mg)仅在最高VTE率(NNT = 131)时具有成本效益,而利伐沙班(20mg)无论如何都不具有成本效益。仅当静脉血栓栓塞治疗费用分别超过5万美元和150万美元时,依诺肝素和利伐沙班才具有成本效益。接受预防治疗的患者出血率(0.56% vs 0.26%)和输血率(0.82% vs 0.25%)较高(P)。结论:本研究发现阿司匹林81 mg、阿司匹林325 mg和华法林对踝关节骨折固定后静脉血栓栓塞化疗预防具有成本效益。依诺肝素和利伐沙班通常不具有成本效益,仅适用于高危患者。证据等级:四级,经济分析。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


