Anna M Gerritsma, Quint A J Hagdorn, Timon H Geurkink, Jan G Groothuis, Clara E E van Ofwegen-Hanekamp, Jurjen S Lagas
{"title":"Dietary lifestyle changes unexpectedly causing digoxin intoxication with cardiogenic shock: a grand round case report.","authors":"Anna M Gerritsma, Quint A J Hagdorn, Timon H Geurkink, Jan G Groothuis, Clara E E van Ofwegen-Hanekamp, Jurjen S Lagas","doi":"10.1093/ehjcr/ytaf352","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Digoxin is primarily used for atrial arrhythmias and known for its narrow therapeutic index. It is predominantly excreted renally and has a long half-life and large volume of distribution, requiring personalized dosing. Due to its narrow therapeutic index, only modestly elevated plasma levels may already cause digoxin toxicity, including gastro-intestinal, ocular, neuropsychiatric, and cardiac complications.</p><p><strong>Case summary: </strong>A 66-year-old Caucasian male, with a history of heart failure with preserved ejection fraction and permanent atrial fibrillation, treated with digoxin 0.25 mg daily and metoprolol succinate 200 mg daily presented to the emergency room. He was in cardiogenic shock due to bradycardia resulting from third-degree AV block with varying escape rhythm (minimum of 20 b.p.m.). A temporary external pacemaker lead was placed. Elevated digoxin serum levels (3.2-3.4 µg/L, toxicity threshold > 2.0 µg/L) and hyperkalaemia were found. To reverse digoxin toxicity, digoxin-specific antibody fragments (digoxin-Fabs) were administered and complete recovery of AV-conduction was observed. Interestingly, the patient recently drastically altered his diet and completely abandoned from massive cola and beer intake.</p><p><strong>Discussion: </strong>The cause of this intoxication is probably multifactorial, including reduced renal digoxin excretion, co-medication, and most likely changes in diet. We hypothesize that this dietary change not only led to substantial weight loss but also resulted in an increase of intragastric pH, thereby significantly enhancing digoxin uptake. This case underscores the importance of considering digoxin-Fabs treatment based on several factors including clinical presentation and digoxin serum levels. Furthermore, it highlights the importance of regular lifestyle anamnesis and renal function assessment to reassess digoxin dosage.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 8","pages":"ytaf352"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12363453/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf352","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
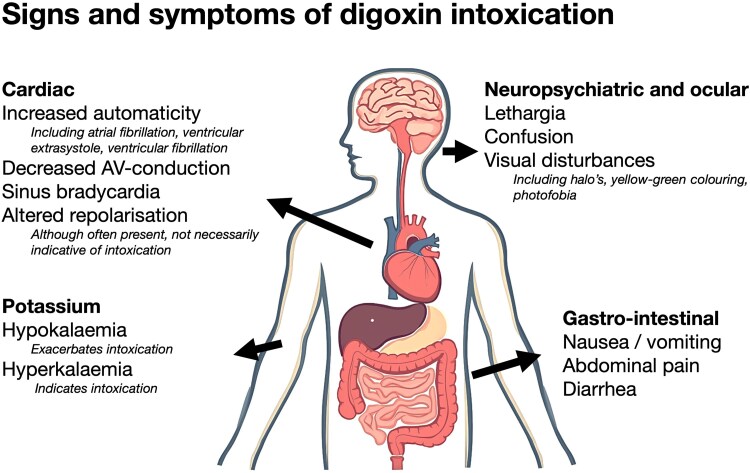
Background: Digoxin is primarily used for atrial arrhythmias and known for its narrow therapeutic index. It is predominantly excreted renally and has a long half-life and large volume of distribution, requiring personalized dosing. Due to its narrow therapeutic index, only modestly elevated plasma levels may already cause digoxin toxicity, including gastro-intestinal, ocular, neuropsychiatric, and cardiac complications.
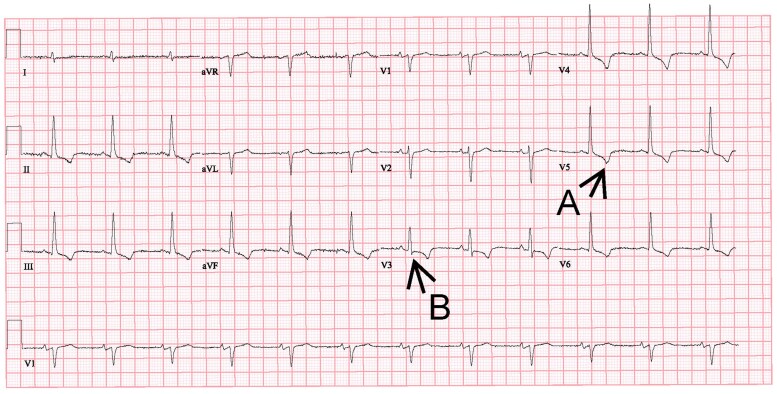
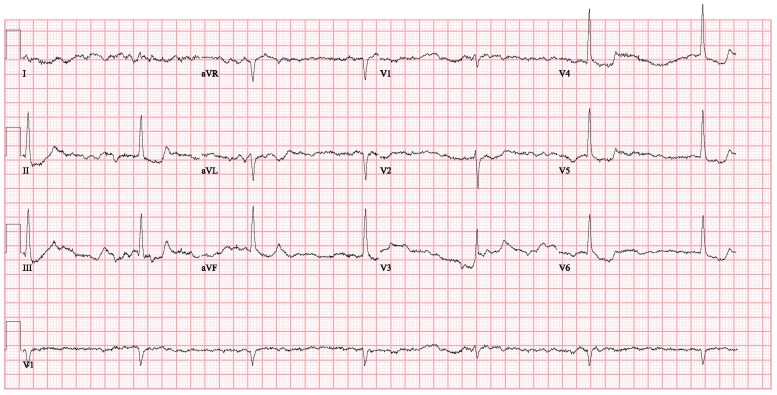
Case summary: A 66-year-old Caucasian male, with a history of heart failure with preserved ejection fraction and permanent atrial fibrillation, treated with digoxin 0.25 mg daily and metoprolol succinate 200 mg daily presented to the emergency room. He was in cardiogenic shock due to bradycardia resulting from third-degree AV block with varying escape rhythm (minimum of 20 b.p.m.). A temporary external pacemaker lead was placed. Elevated digoxin serum levels (3.2-3.4 µg/L, toxicity threshold > 2.0 µg/L) and hyperkalaemia were found. To reverse digoxin toxicity, digoxin-specific antibody fragments (digoxin-Fabs) were administered and complete recovery of AV-conduction was observed. Interestingly, the patient recently drastically altered his diet and completely abandoned from massive cola and beer intake.
Discussion: The cause of this intoxication is probably multifactorial, including reduced renal digoxin excretion, co-medication, and most likely changes in diet. We hypothesize that this dietary change not only led to substantial weight loss but also resulted in an increase of intragastric pH, thereby significantly enhancing digoxin uptake. This case underscores the importance of considering digoxin-Fabs treatment based on several factors including clinical presentation and digoxin serum levels. Furthermore, it highlights the importance of regular lifestyle anamnesis and renal function assessment to reassess digoxin dosage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


