Merve Kural, Stephan Rosenkranz, Stephan Baldus, Alexander Christian Bunck, Tobias Tichelbäcker
{"title":"In-hospital cardiac arrest due to acute pulmonary embolism: a case report of successful catheter-directed thrombectomy on a patient with VA-ECMO.","authors":"Merve Kural, Stephan Rosenkranz, Stephan Baldus, Alexander Christian Bunck, Tobias Tichelbäcker","doi":"10.1093/ehjcr/ytaf342","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>First-line therapy for high-risk pulmonary embolism (PE) is systemic thrombolysis. Catheter-directed thrombectomy (CDT) poses as a secondary option, primarily in patients with contraindications for systemic thrombolysis. However, in patients with haemodynamic instability or cardiac arrest, CDT can worsen the haemodynamic situation making use of large thrombectomy catheters. The implementation of extracorporeal life support such as veno-arterial extracorporeal membrane oxygenation (VA-ECMO) can play a decisive role in making CDT possible. Herein, we present a case of CDT on a high-risk PE patient under VA-ECMO.</p><p><strong>Case summary: </strong>A 73-year-old White male was hospitalized in order to perform abdominal surgery. Afterwards, multiple complications led to recurring operations and a prolonged immobilization time. In the aftermath, the patient suffered an in-hospital cardiac arrest and was put on VA-ECMO. A computed tomography pulmonary angiography presented bilateral central PE. Due to contraindications for systemic thrombolysis, successful CDT using a FlowTriever catheter was performed, leading to a reduction of mean pulmonary arterial pressure. ECMO therapy could be terminated in the following days. The patient was eventually discharged without any signs of right heart strain in transthoracic echocardiogram, neurological sequelae or dyspnoea.</p><p><strong>Discussion: </strong>According to current ESC-guidelines, first-line therapy for high-risk PE is systemic thrombolysis, and CDT is a secondary option. In our case, CDT under VA-ECMO was feasible and led to a rapid improvement in haemodynamics, resulting in a long-term recovery. Thus, the definite significance of CDT has yet to be identified, especially concerning PE with refractory cardiac arrest and contraindications for systemic thrombolysis.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 8","pages":"ytaf342"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377017/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf342","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: First-line therapy for high-risk pulmonary embolism (PE) is systemic thrombolysis. Catheter-directed thrombectomy (CDT) poses as a secondary option, primarily in patients with contraindications for systemic thrombolysis. However, in patients with haemodynamic instability or cardiac arrest, CDT can worsen the haemodynamic situation making use of large thrombectomy catheters. The implementation of extracorporeal life support such as veno-arterial extracorporeal membrane oxygenation (VA-ECMO) can play a decisive role in making CDT possible. Herein, we present a case of CDT on a high-risk PE patient under VA-ECMO.
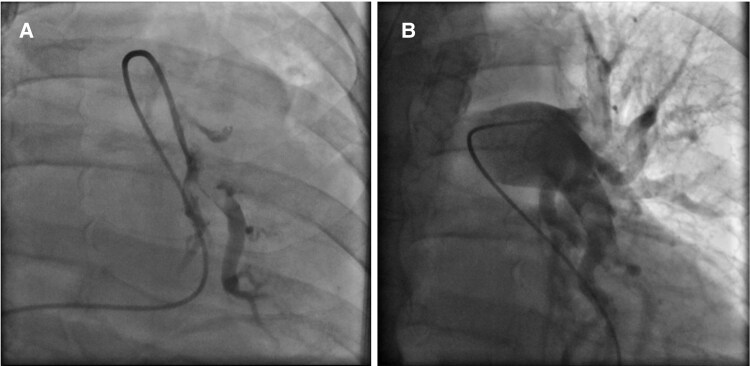
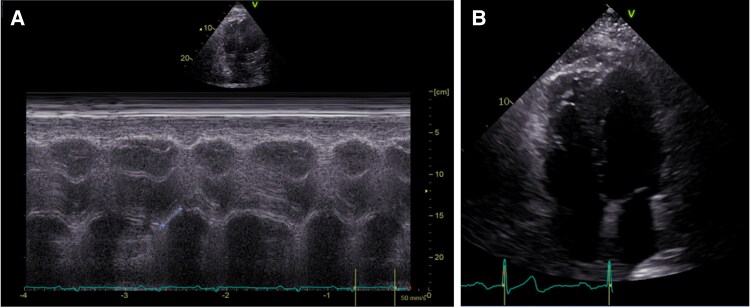
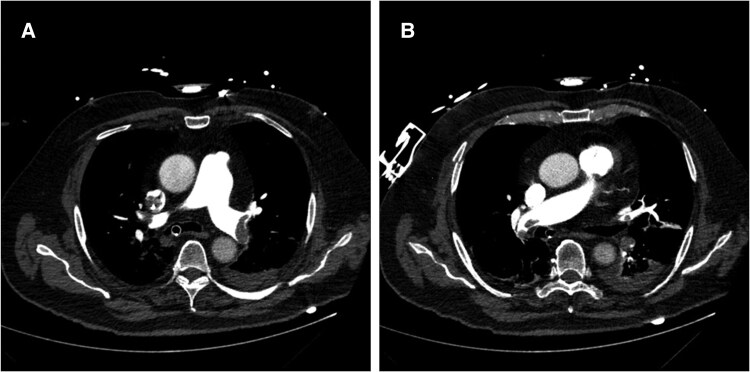
Case summary: A 73-year-old White male was hospitalized in order to perform abdominal surgery. Afterwards, multiple complications led to recurring operations and a prolonged immobilization time. In the aftermath, the patient suffered an in-hospital cardiac arrest and was put on VA-ECMO. A computed tomography pulmonary angiography presented bilateral central PE. Due to contraindications for systemic thrombolysis, successful CDT using a FlowTriever catheter was performed, leading to a reduction of mean pulmonary arterial pressure. ECMO therapy could be terminated in the following days. The patient was eventually discharged without any signs of right heart strain in transthoracic echocardiogram, neurological sequelae or dyspnoea.
Discussion: According to current ESC-guidelines, first-line therapy for high-risk PE is systemic thrombolysis, and CDT is a secondary option. In our case, CDT under VA-ECMO was feasible and led to a rapid improvement in haemodynamics, resulting in a long-term recovery. Thus, the definite significance of CDT has yet to be identified, especially concerning PE with refractory cardiac arrest and contraindications for systemic thrombolysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


