Lac Duy Le, Binh Duc Doan, Anh Thai Nguyen, Tri Cong Le, Thanh Tri Vu
{"title":"Concurrent inferior stemi with third-degree AV block and acute intracranial haemorrhage: how we overcame this clinical challenge-a case report.","authors":"Lac Duy Le, Binh Duc Doan, Anh Thai Nguyen, Tri Cong Le, Thanh Tri Vu","doi":"10.1093/ehjcr/ytaf385","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The concurrent management of ST-elevation myocardial infarction (STEMI) and acute intracerebral haemorrhage (ICH) poses a significant clinical challenge due to conflicting treatment goals. While the management of STEMI requires coronary reperfusion with antithrombotic agents (anticoagulants and antiplatelets), such treatments are contraindicated in cases of ICH. The coexistence of STEMI and ICH is exceedingly rare in the literature and is associated with high mortality rates. Furthermore, no specific guidelines currently exist for managing such cases.</p><p><strong>Case summary: </strong>We report a case of a 67-year-old male presenting with acute ICH who subsequently developed inferior STEMI complicated by third-degree atrioventricular block. The patient underwent a deferred percutaneous coronary intervention (PCI) strategy, involving only balloon angioplasty and thrombectomy without stent placement, to restore coronary flow while minimizing the risk of exacerbating the intracranial haemorrhage. Three days later, ischaemia progressed to recurrent myocardial infarction, at which point reassessment revealed stabilization of the ICH, allowing for stent placement in the right coronary artery (RCA) and the administration of antithrombotic therapy.</p><p><strong>Discussion: </strong>The deferred PCI strategy, involving initial thrombectomy and balloon angioplasty without stent placement, facilitated temporary restoration of coronary flow and provided a critical time window for the stabilization of the ICH. This approach enabled subsequent stent implantation and the reintroduction of antithrombotic therapy (anticoagulants and antiplatelets). This strategy demonstrates its effectiveness in managing patients with concurrent STEMI and ICH by balancing the risks of ischaemia and haemorrhage, thereby improving clinical outcomes.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 8","pages":"ytaf385"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12368336/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf385","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The concurrent management of ST-elevation myocardial infarction (STEMI) and acute intracerebral haemorrhage (ICH) poses a significant clinical challenge due to conflicting treatment goals. While the management of STEMI requires coronary reperfusion with antithrombotic agents (anticoagulants and antiplatelets), such treatments are contraindicated in cases of ICH. The coexistence of STEMI and ICH is exceedingly rare in the literature and is associated with high mortality rates. Furthermore, no specific guidelines currently exist for managing such cases.
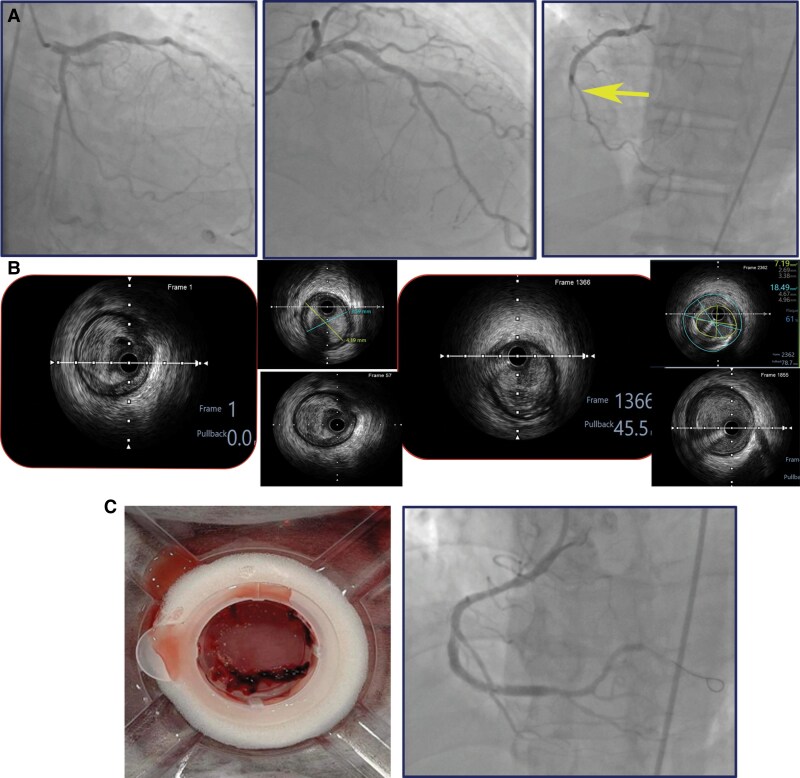
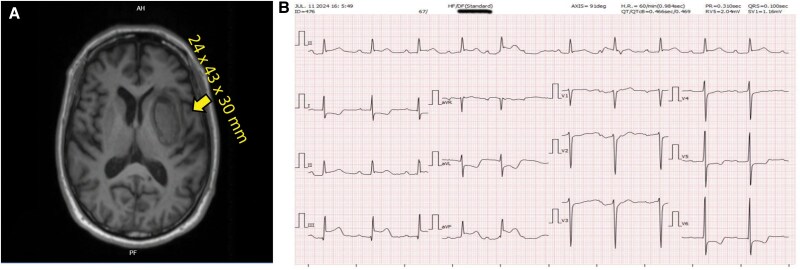
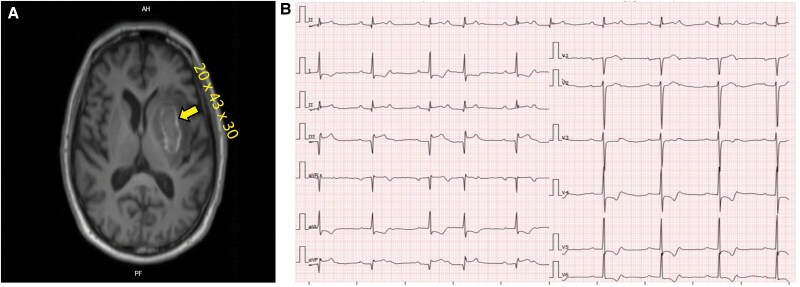
Case summary: We report a case of a 67-year-old male presenting with acute ICH who subsequently developed inferior STEMI complicated by third-degree atrioventricular block. The patient underwent a deferred percutaneous coronary intervention (PCI) strategy, involving only balloon angioplasty and thrombectomy without stent placement, to restore coronary flow while minimizing the risk of exacerbating the intracranial haemorrhage. Three days later, ischaemia progressed to recurrent myocardial infarction, at which point reassessment revealed stabilization of the ICH, allowing for stent placement in the right coronary artery (RCA) and the administration of antithrombotic therapy.
Discussion: The deferred PCI strategy, involving initial thrombectomy and balloon angioplasty without stent placement, facilitated temporary restoration of coronary flow and provided a critical time window for the stabilization of the ICH. This approach enabled subsequent stent implantation and the reintroduction of antithrombotic therapy (anticoagulants and antiplatelets). This strategy demonstrates its effectiveness in managing patients with concurrent STEMI and ICH by balancing the risks of ischaemia and haemorrhage, thereby improving clinical outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


