{"title":"Optimal endoscopic resection method based on vertical margin distance for small rectal neuroendocrine tumors: Propensity score-matched study.","authors":"Jianning Liu, Weihua Yu, Peng Liu, Hao Tian, Lihong Gan, Kaige Zhang, Hui Chen, Nian Fang","doi":"10.1055/a-2655-1320","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and study aims: </strong>Advanced endoscopic resection methods are recommended for removing rectal neuroendocrine tumors (NETs) < 10 mm, but there is no consensus on optimal endoscopic technique. This study aimed to determine whether endoscopic mucosal resection with ligation (EMR-L) is superior to endoscopic submucosal dissection (ESD) in terms of efficacy and safety, focusing on achieving adequate vertical margin distance.</p><p><strong>Patients and methods: </strong>This dual-center cohort study included consecutive patients with rectal NETs ≤ 10 mm. Adequate vertical margins were exploratively defined as a margin distance exceeding 115 μm, the 25th percentile threshold. Propensity score matching (PSM) was applied to compare outcomes between EMR-L and ESD.</p><p><strong>Results: </strong>The study included 204 rectal NETs from 186 patients, with 61 lesions in each group after PSM. Compared with ESD, the EMR-L group demonstrated a higher R0 resection rate (98.4% vs. 83.6%, <i>P</i> = 0.021), a greater proportion of adequate vertical margins (80.3% vs. 62.3%, <i>P</i> = 0.030), and a lower rate of positive vertical margins (1.6% vs. 13.1%, <i>P</i> = 0.041). Subgroup analysis indicated that lesions ≤ 5 mm without prior biopsy or central depression derived greater benefit from EMR-L. Furthermore, EMR-L was associated with significantly shorter procedure times (median 5.0 vs. 19 minutes) and a markedly lower overall complication rate (8.2% vs. 29.5%, <i>P</i> = 0.005), particularly perforation (3.3% vs. 16.4%, <i>P</i> = 0.028).</p><p><strong>Conclusions: </strong>EMR-L outperforms ESD for small rectal NETs by achieving higher R0 and better vertical margins in shorter times, while minimizing risk of perforation.</p>","PeriodicalId":11671,"journal":{"name":"Endoscopy International Open","volume":"13 ","pages":"a26551320"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12371650/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endoscopy International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2655-1320","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and study aims: Advanced endoscopic resection methods are recommended for removing rectal neuroendocrine tumors (NETs) < 10 mm, but there is no consensus on optimal endoscopic technique. This study aimed to determine whether endoscopic mucosal resection with ligation (EMR-L) is superior to endoscopic submucosal dissection (ESD) in terms of efficacy and safety, focusing on achieving adequate vertical margin distance.
Patients and methods: This dual-center cohort study included consecutive patients with rectal NETs ≤ 10 mm. Adequate vertical margins were exploratively defined as a margin distance exceeding 115 μm, the 25th percentile threshold. Propensity score matching (PSM) was applied to compare outcomes between EMR-L and ESD.
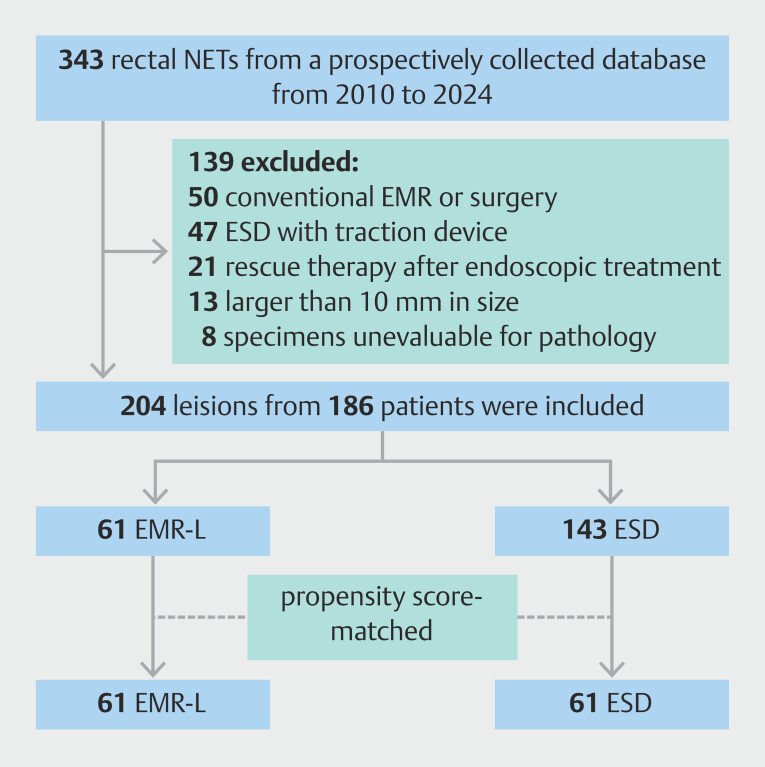
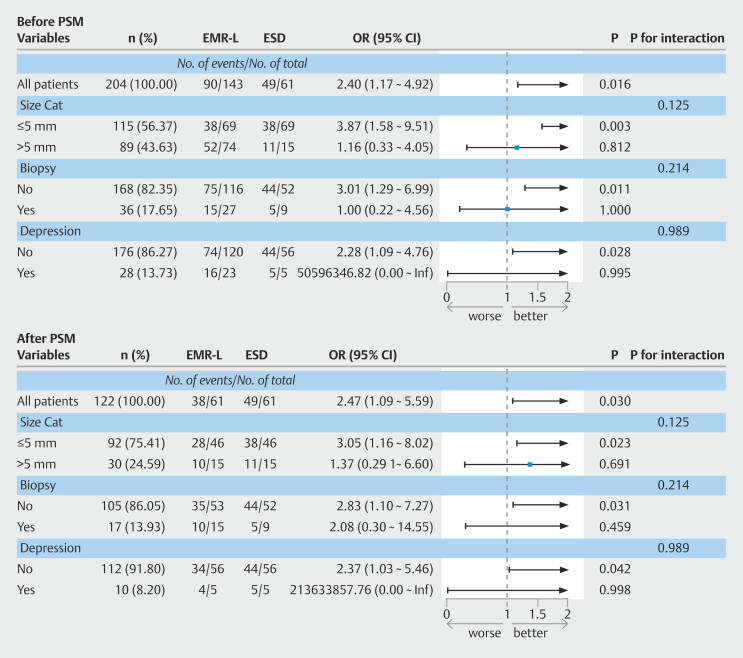
Results: The study included 204 rectal NETs from 186 patients, with 61 lesions in each group after PSM. Compared with ESD, the EMR-L group demonstrated a higher R0 resection rate (98.4% vs. 83.6%, P = 0.021), a greater proportion of adequate vertical margins (80.3% vs. 62.3%, P = 0.030), and a lower rate of positive vertical margins (1.6% vs. 13.1%, P = 0.041). Subgroup analysis indicated that lesions ≤ 5 mm without prior biopsy or central depression derived greater benefit from EMR-L. Furthermore, EMR-L was associated with significantly shorter procedure times (median 5.0 vs. 19 minutes) and a markedly lower overall complication rate (8.2% vs. 29.5%, P = 0.005), particularly perforation (3.3% vs. 16.4%, P = 0.028).
Conclusions: EMR-L outperforms ESD for small rectal NETs by achieving higher R0 and better vertical margins in shorter times, while minimizing risk of perforation.
背景与研究目的:对于< 10 mm的直肠神经内分泌肿瘤(NETs),建议采用先进的内镜切除方法,但对最佳内镜技术尚无共识。本研究旨在确定内镜下粘膜结扎切除术(EMR-L)是否优于内镜下粘膜剥离术(ESD)的有效性和安全性,重点关注是否能获得足够的垂直切缘距离。患者和方法:这项双中心队列研究包括直肠NETs≤10 mm的连续患者。适当的垂直边缘被探索性地定义为边缘距离超过115 μm,即第25个百分位阈值。倾向评分匹配(PSM)用于比较EMR-L和ESD的结果。结果:本研究纳入186例204例直肠NETs,每组经PSM后病变61个。与ESD组相比,EMR-L组的R0切除率更高(98.4%比83.6%,P = 0.021),垂直切缘充足的比例更高(80.3%比62.3%,P = 0.030),垂直切缘阳性的比例更低(1.6%比13.1%,P = 0.041)。亚组分析表明,病变≤5mm且没有事先活检或中枢性凹陷的患者从EMR-L中获益更大。此外,EMR-L显著缩短了手术时间(中位数5.0 vs 19分钟),显著降低了总并发症发生率(8.2% vs 29.5%, P = 0.005),尤其是穿孔(3.3% vs 16.4%, P = 0.028)。结论:EMR-L优于ESD,在更短的时间内获得更高的R0和更好的垂直切缘,同时最大限度地降低了穿孔的风险。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


