Samuel Truniger, Jan Borovicka, Marius König, Michael Bento Schmid, Nicola Fabian Frei, Stephan Brand
{"title":"First Description of Upadacitinib as Treatment for Collagenous Colitis with a Concomitant Lymphocytic Disorder of the Upper Gastrointestinal Tract.","authors":"Samuel Truniger, Jan Borovicka, Marius König, Michael Bento Schmid, Nicola Fabian Frei, Stephan Brand","doi":"10.1159/000543901","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The medical treatment of refractory collagenous colitis with a concomitant symptomatic lymphocytic disorder of the upper gastrointestinal tract is very challenging with scarce evidence.</p><p><strong>Case presentation: </strong>We present a 61-year-old female patient with a long-standing highly refractory collagenous colitis with a concomitant symptomatic lymphocytic disorder with villous atrophy and intraepithelial lymphocytes of the upper gastrointestinal tract causing severe watery diarrhoea with severe hypokalemia and recurrent episodes of prerenal kidney injuries requiring several hospital admissions. Celiac serology as well as genetic analyses (HLA-DQ2/DQ8) were negative, and other common etiologies of intraepithelial lymphocytosis and villous atrophy were ruled out. Considering the similar course of the disease in the upper and lower gastrointestinal tract for a time period of more than 20 years, a common etiologic relationship, particularly an autoimmune disorder seems to be very likely in this patient. Several therapies such as budesonide, immunomodulators, and the biologics infliximab and vedolizumab had to be stopped due to either non-response, loss-of-response or drug-related side effects. However, the patient responded immediately to the JAK-1 inhibitor upadacitinib, with documented remission for more than 1 year.</p><p><strong>Conclusion: </strong>For the first time, a prompt and significant response to upadacitinib in a patient with refractory collagenous colitis with upper gastrointestinal tract involvement was shown, suggesting upadacitinib as therapy of choice in severe therapy-refractory cases of collagenous colitis, particularly with concomitant upper gastrointestinal tract involvement.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"204-210"},"PeriodicalIF":0.6000,"publicationDate":"2025-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11942591/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543901","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The medical treatment of refractory collagenous colitis with a concomitant symptomatic lymphocytic disorder of the upper gastrointestinal tract is very challenging with scarce evidence.
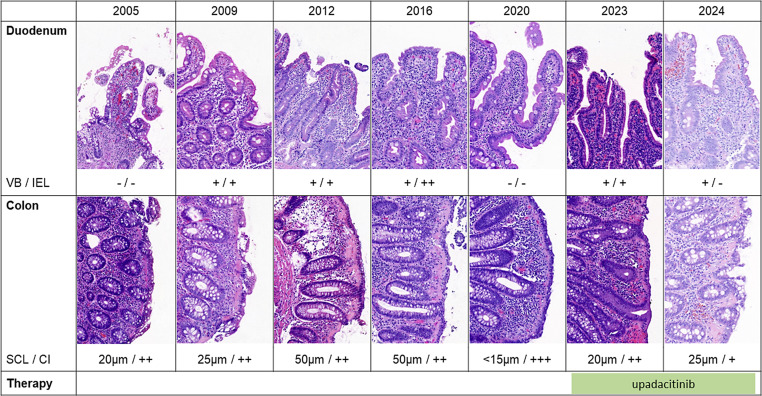
Case presentation: We present a 61-year-old female patient with a long-standing highly refractory collagenous colitis with a concomitant symptomatic lymphocytic disorder with villous atrophy and intraepithelial lymphocytes of the upper gastrointestinal tract causing severe watery diarrhoea with severe hypokalemia and recurrent episodes of prerenal kidney injuries requiring several hospital admissions. Celiac serology as well as genetic analyses (HLA-DQ2/DQ8) were negative, and other common etiologies of intraepithelial lymphocytosis and villous atrophy were ruled out. Considering the similar course of the disease in the upper and lower gastrointestinal tract for a time period of more than 20 years, a common etiologic relationship, particularly an autoimmune disorder seems to be very likely in this patient. Several therapies such as budesonide, immunomodulators, and the biologics infliximab and vedolizumab had to be stopped due to either non-response, loss-of-response or drug-related side effects. However, the patient responded immediately to the JAK-1 inhibitor upadacitinib, with documented remission for more than 1 year.
Conclusion: For the first time, a prompt and significant response to upadacitinib in a patient with refractory collagenous colitis with upper gastrointestinal tract involvement was shown, suggesting upadacitinib as therapy of choice in severe therapy-refractory cases of collagenous colitis, particularly with concomitant upper gastrointestinal tract involvement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


