{"title":"Echocardiographic measurement of inferior vena cava diameter for estimating central venous pressure in adult Fontan patients.","authors":"Makoto Miyake, Hiraku Doi, Yu Noguchi, Kyokun Uehara, Toshihiro Tamura","doi":"10.1093/ehjimp/qyaf089","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>In adult Fontan patients, a higher central venous pressure (CVP) is associated with worse clinical outcomes. Assessing CVP is helpful to guide therapeutic strategies; however, it remains unclear whether CVP can be accurately estimated from the inferior vena cava (IVC) diameter by echocardiography.</p><p><strong>Methods and results: </strong>This single-centre, retrospective study enrolled 21 adult Fontan patients (median age: 21.5 years, 52% male) who had a transthoracic echocardiogram performed after admission for a scheduled cardiac catheterization. The relationship between CVP estimated by echocardiography and CVP measured by catheterization was investigated. According to echocardiographic guidelines, CVP was estimated to be 3, 8, or 15 mmHg on the basis of the IVC diameter and its respiratory collapse. To evaluate the agreement between estimated and measured CVP grades, measured CVP was also classified into three grades. The mean IVC diameter and measured CVP were 1.41 ± 0.27 cm and 11.9 ± 2.8 mmHg, respectively. Both the IVC diameter and the estimated CVP grade were correlated with measured CVP (<i>r</i> = 0.526, <i>P</i> = 0.014 and rho = 0.573, <i>P</i> = 0.007, respectively). However, the estimated CVP grade was concordant with the measured CVP grade in only two patients. In the remaining 19 patients (90%), the estimated CVP grade was lower than the measured CVP grade. Only slight agreement was observed between these two gradings of CVP [weighted kappa coefficient: 0.13, 95% confidence interval (CI): 0.00-0.25].</p><p><strong>Conclusion: </strong>In adult Fontan patients, the echocardiographic classification of CVP grading using the IVC diameter may underestimate CVP, suggesting that this echocardiographic method cannot replace invasive methods in accurately assessing CVP.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"3 3","pages":"qyaf089"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12360295/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyaf089","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
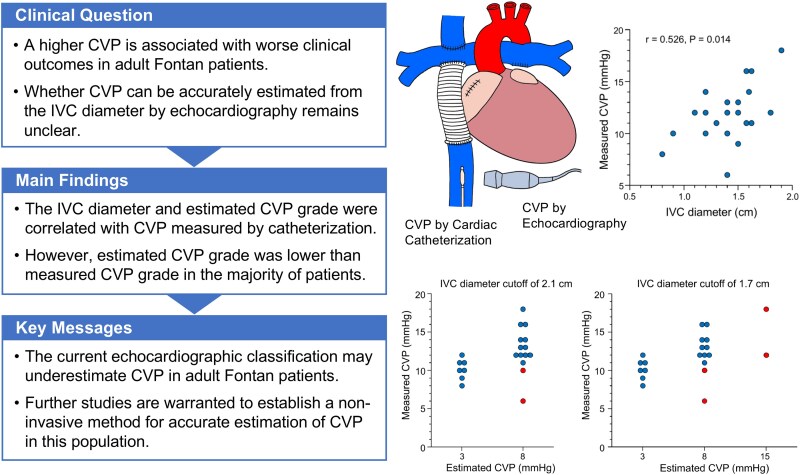
Aims: In adult Fontan patients, a higher central venous pressure (CVP) is associated with worse clinical outcomes. Assessing CVP is helpful to guide therapeutic strategies; however, it remains unclear whether CVP can be accurately estimated from the inferior vena cava (IVC) diameter by echocardiography.
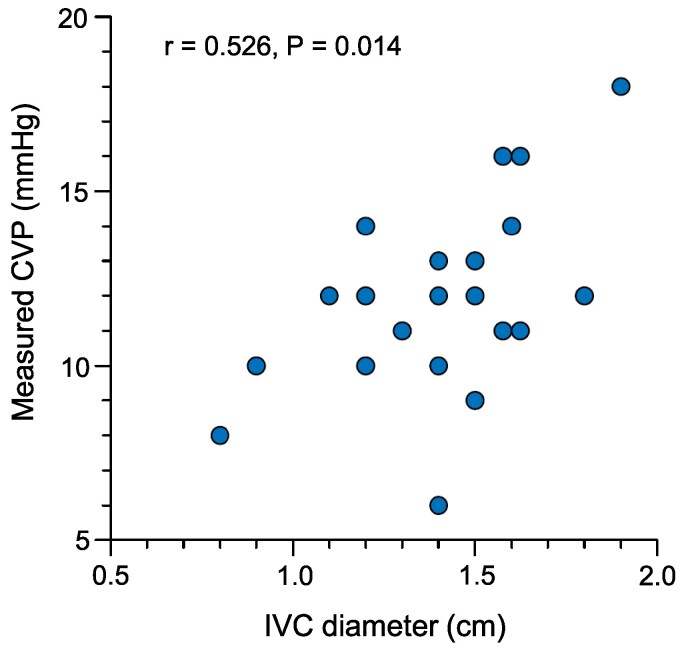
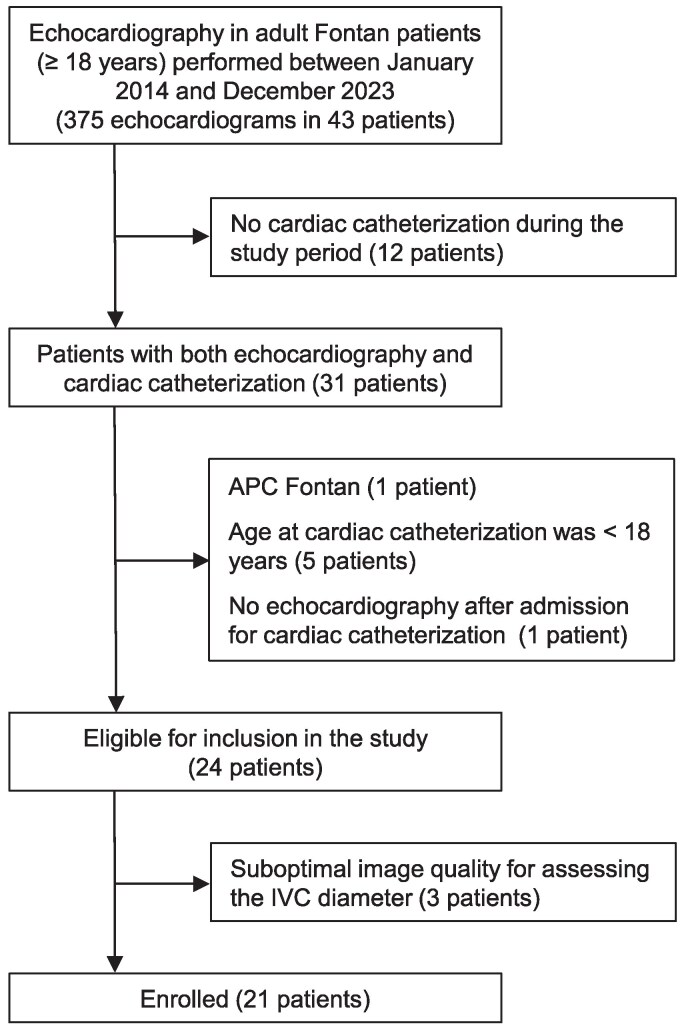
Methods and results: This single-centre, retrospective study enrolled 21 adult Fontan patients (median age: 21.5 years, 52% male) who had a transthoracic echocardiogram performed after admission for a scheduled cardiac catheterization. The relationship between CVP estimated by echocardiography and CVP measured by catheterization was investigated. According to echocardiographic guidelines, CVP was estimated to be 3, 8, or 15 mmHg on the basis of the IVC diameter and its respiratory collapse. To evaluate the agreement between estimated and measured CVP grades, measured CVP was also classified into three grades. The mean IVC diameter and measured CVP were 1.41 ± 0.27 cm and 11.9 ± 2.8 mmHg, respectively. Both the IVC diameter and the estimated CVP grade were correlated with measured CVP (r = 0.526, P = 0.014 and rho = 0.573, P = 0.007, respectively). However, the estimated CVP grade was concordant with the measured CVP grade in only two patients. In the remaining 19 patients (90%), the estimated CVP grade was lower than the measured CVP grade. Only slight agreement was observed between these two gradings of CVP [weighted kappa coefficient: 0.13, 95% confidence interval (CI): 0.00-0.25].
Conclusion: In adult Fontan patients, the echocardiographic classification of CVP grading using the IVC diameter may underestimate CVP, suggesting that this echocardiographic method cannot replace invasive methods in accurately assessing CVP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


