Joshua D Gazzetta, Poster P Mutambo, Mutimba B Mpabalwani, Mwamba Jc Mulenga, Cyrus Phiri, Kelvin Shaba, Emmanuel M Makasa
{"title":"The Implementation of a Perioperative Registry in a Resource-Limited Setting: A Feasibility, Fidelity, and Acceptance Study.","authors":"Joshua D Gazzetta, Poster P Mutambo, Mutimba B Mpabalwani, Mwamba Jc Mulenga, Cyrus Phiri, Kelvin Shaba, Emmanuel M Makasa","doi":"10.18103/mra.v13i6.6574","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In low and middle-income countries, nine out of every ten persons is unable to access safe and timely surgery. The limited perioperative data in resource-limited settings compromises surgical and research capacity growth. By increasing data availability, surgical disparities may be addressed through research efforts and quality initiatives. This project aimed to implement and evaluate a perioperative registry in a tertiary care hospital in a low-income country.</p><p><strong>Methods: </strong>A prospective emergency laparotomy perioperative registry was implemented in Zambia's largest teaching and referral hospital. Over the first 6-months of implementation, 162 patients were included. Data was collected postoperatively, before discharge, and at 30 days. The registries feasibility was assessed by evaluating patient accrual, retention, and 30-day completion rates. The registries fidelity was measured by evaluating data missingness. A participant acceptance survey was retrospectively collected and analyzed for the first 25 consecutively enrolled patients.</p><p><strong>Results: </strong>The capture rate of the registry could not be calculated due to a destroyed theatre logbook. The participant accrual and retention rates were 99.4% and 95.1%, respectively. The participant completion rate at 30-days was 75.6%. The overall incidence of missing information in the registry was 3.5%. More than 75% of participant responses to the acceptance survey were positive in each category regarding the ethical conduct of research and the storing of personal data.</p><p><strong>Conclusion: </strong>The value of this study is the reporting and evaluation of a successful perioperative registry implementation with minimal external funding. This framework is being used to develop new data registries and may provide a roadmap for other hospitals with resource constraints.</p>","PeriodicalId":94137,"journal":{"name":"Medical research archives","volume":"13 6","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12360225/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical research archives","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18103/mra.v13i6.6574","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In low and middle-income countries, nine out of every ten persons is unable to access safe and timely surgery. The limited perioperative data in resource-limited settings compromises surgical and research capacity growth. By increasing data availability, surgical disparities may be addressed through research efforts and quality initiatives. This project aimed to implement and evaluate a perioperative registry in a tertiary care hospital in a low-income country.
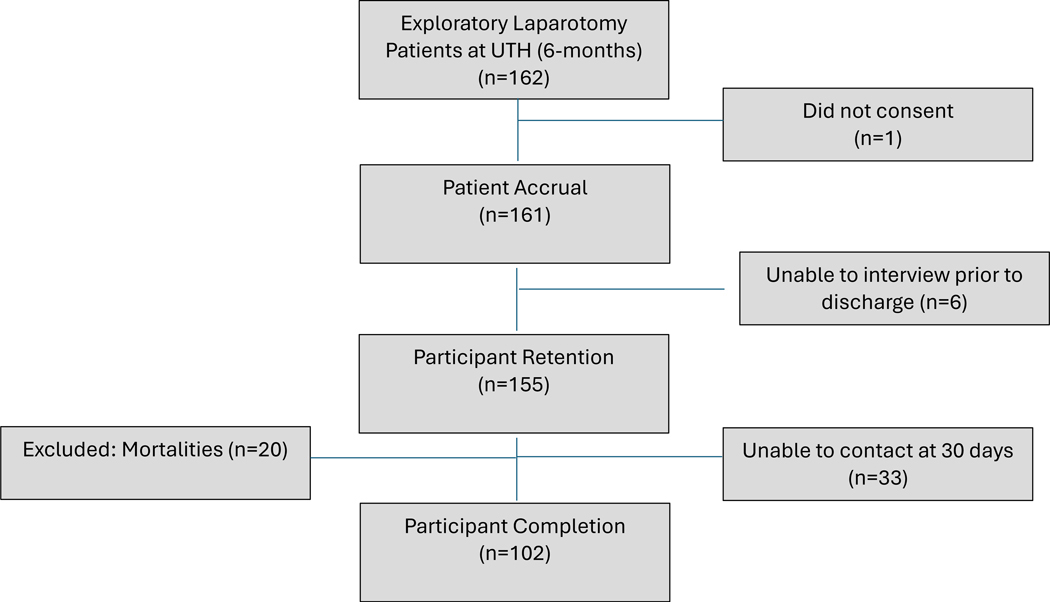
Methods: A prospective emergency laparotomy perioperative registry was implemented in Zambia's largest teaching and referral hospital. Over the first 6-months of implementation, 162 patients were included. Data was collected postoperatively, before discharge, and at 30 days. The registries feasibility was assessed by evaluating patient accrual, retention, and 30-day completion rates. The registries fidelity was measured by evaluating data missingness. A participant acceptance survey was retrospectively collected and analyzed for the first 25 consecutively enrolled patients.
Results: The capture rate of the registry could not be calculated due to a destroyed theatre logbook. The participant accrual and retention rates were 99.4% and 95.1%, respectively. The participant completion rate at 30-days was 75.6%. The overall incidence of missing information in the registry was 3.5%. More than 75% of participant responses to the acceptance survey were positive in each category regarding the ethical conduct of research and the storing of personal data.
Conclusion: The value of this study is the reporting and evaluation of a successful perioperative registry implementation with minimal external funding. This framework is being used to develop new data registries and may provide a roadmap for other hospitals with resource constraints.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


