{"title":"S3 sacral-alar iliac screws application in partial sacral resection for an aneurysmal bone cyst: illustrative case.","authors":"Hudin N Jackson, Thomas Hamre, David F Bauer","doi":"10.3171/CASE25267","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sacropelvic fixation is used in the management of deformity, neoplasms, and fractures. S2-alar-iliac (S2AI) screws have evolved as a technique for sacropelvic fixation to address disadvantages associated with traditional iliac screws. In select patients, S2AI screw placement is not feasible due to patient anatomy, trauma, or osteolytic lesions.</p><p><strong>Observations: </strong>A 15-year-old girl presented with a 3-month history of right S1-2 radicular pain and right dorsiflexion and plantar flexion weakness. Imaging revealed a right sacral alar aneurysmal bone cyst. The patient underwent right S1-3 hemilaminectomies and partial resection of the S2 and S3 vertebral bodies. Following adequate bony decompression, tumor debulking was performed. Bilateral L4-S1 pedicle screws and left S2AI screws were then placed using neuronavigation guidance. Due to right S1-2 sacral resection, S2AI screw placement was unfeasible. Right-S3 alar-iliac (S3AI) screw placement was performed, and good sacropelvic fixation was demonstrated. Herein, the authors describe the first clinical application of S3AI screw placement in a pediatric patient. After surgery, the patient experienced an improvement in symptoms before later tumor recurrence, which required adjuvant therapy. Long term follow-up revealed solid fusion with stable spinal alignment.</p><p><strong>Lessons: </strong>In select patients in whom S2AI screw placement is not an option, S3AI screw placement is a feasible, safe, alternative for sacropelvic fixation. https://thejns.org/doi/10.3171/CASE25267.</p>","PeriodicalId":94098,"journal":{"name":"Journal of neurosurgery. Case lessons","volume":"10 7","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12362192/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of neurosurgery. Case lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE25267","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sacropelvic fixation is used in the management of deformity, neoplasms, and fractures. S2-alar-iliac (S2AI) screws have evolved as a technique for sacropelvic fixation to address disadvantages associated with traditional iliac screws. In select patients, S2AI screw placement is not feasible due to patient anatomy, trauma, or osteolytic lesions.
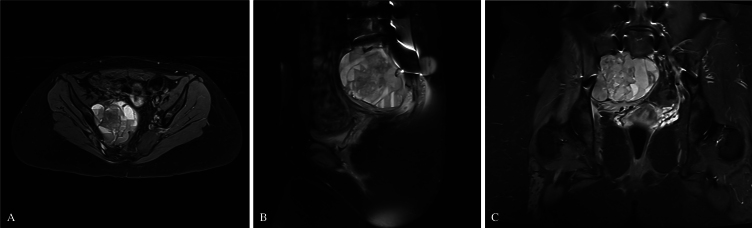
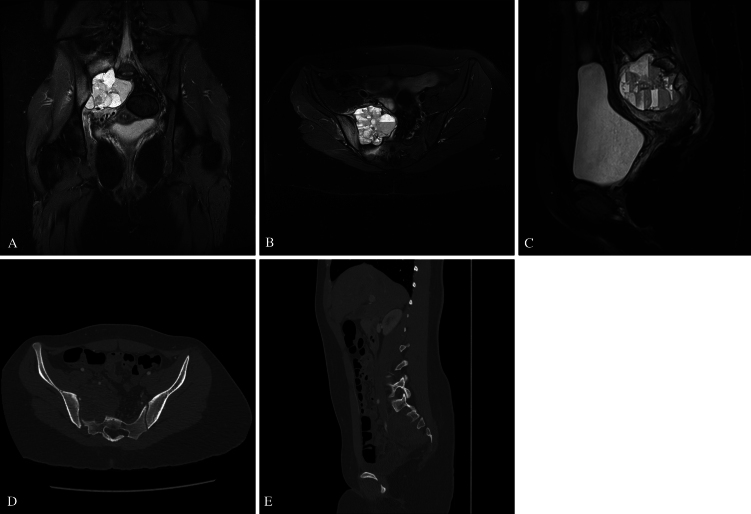
Observations: A 15-year-old girl presented with a 3-month history of right S1-2 radicular pain and right dorsiflexion and plantar flexion weakness. Imaging revealed a right sacral alar aneurysmal bone cyst. The patient underwent right S1-3 hemilaminectomies and partial resection of the S2 and S3 vertebral bodies. Following adequate bony decompression, tumor debulking was performed. Bilateral L4-S1 pedicle screws and left S2AI screws were then placed using neuronavigation guidance. Due to right S1-2 sacral resection, S2AI screw placement was unfeasible. Right-S3 alar-iliac (S3AI) screw placement was performed, and good sacropelvic fixation was demonstrated. Herein, the authors describe the first clinical application of S3AI screw placement in a pediatric patient. After surgery, the patient experienced an improvement in symptoms before later tumor recurrence, which required adjuvant therapy. Long term follow-up revealed solid fusion with stable spinal alignment.
Lessons: In select patients in whom S2AI screw placement is not an option, S3AI screw placement is a feasible, safe, alternative for sacropelvic fixation. https://thejns.org/doi/10.3171/CASE25267.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


