Streamlined concomitant pulse field ablation-based pulmonary vein isolation and left atrial appendage occlusion via a single venous access approach: a case report.
Christian-H Heeger, Henning Rolfes, Lena Böttcher, Felix Meincke, Martin W Bergmann
{"title":"Streamlined concomitant pulse field ablation-based pulmonary vein isolation and left atrial appendage occlusion via a single venous access approach: a case report.","authors":"Christian-H Heeger, Henning Rolfes, Lena Böttcher, Felix Meincke, Martin W Bergmann","doi":"10.1093/ehjcr/ytaf350","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pulsed field ablation (PFA) is a novel non-thermal cardiac ablation method utilizing irreversible electroporation which has been introduced especially for treatment of atrial fibrillation (AF) by pulmonary vein isolation (PVI). Interventional left atrial appendage closure (LAAC) is an alternative to oral anticoagulation (OAC) in patients with non-valvular AF and high stroke risk who are ineligible for OAC. A concomitant PVI and LAAC might be beneficial for patients.</p><p><strong>Case summary: </strong>In an 82-year-old male patient with symptomatic persistent AF, CHA<sub>2</sub>DS<sub>2-</sub>VA Score of 4 and HASBLED Score of 3 due to previous gastrointestinal bleeding were scheduled for a concomitant PVI + LAAC procedure. For minimum risk, a streamlined approach utilizing a single femoral vein puncture in combination with a suture-based closure system (Perclose Prostyle, Abbott) was performed. The transoesophageal echocardiography (TOE) LAA landing zone measurements were achieved directly prior ablation. Pulmonary vein isolation was performed with pentaspline PFA catheter (FARAPULSE). Although a swelling of the left atrial ridge was observed, a 24 mm WATCHMAN FLX device was successfully implanted. The patient was mobilized after 2 h and discharged on the next day. After 2 months on OAC, TOE found no gaps or leakage of the LAAC device and OAC was switched to acetylsalicylic acid monotherapy.</p><p><strong>Discussion: </strong>A streamlined concomitant PFA-based PVI and LAAC procedure utilizing FARAPULSE and WATCHMAN FLX devices seems to be feasible and safe. Swelling of the ridge after PVI was observed; however, the sizing measurements have been performed prior PVI, and the LAAC procedure was successful with no evidence for gaps or leakage. A concomitant approach might be a suitable option for selected patients.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 8","pages":"ytaf350"},"PeriodicalIF":0.8000,"publicationDate":"2025-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12352103/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf350","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pulsed field ablation (PFA) is a novel non-thermal cardiac ablation method utilizing irreversible electroporation which has been introduced especially for treatment of atrial fibrillation (AF) by pulmonary vein isolation (PVI). Interventional left atrial appendage closure (LAAC) is an alternative to oral anticoagulation (OAC) in patients with non-valvular AF and high stroke risk who are ineligible for OAC. A concomitant PVI and LAAC might be beneficial for patients.
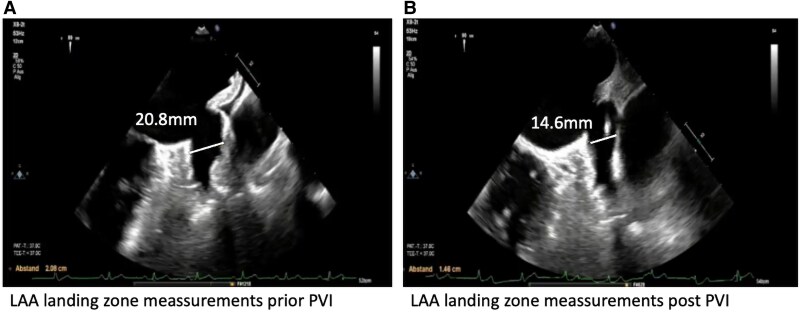
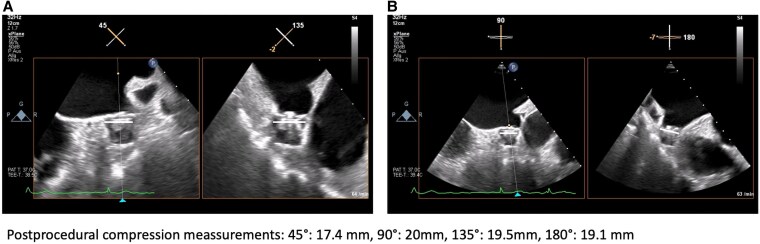
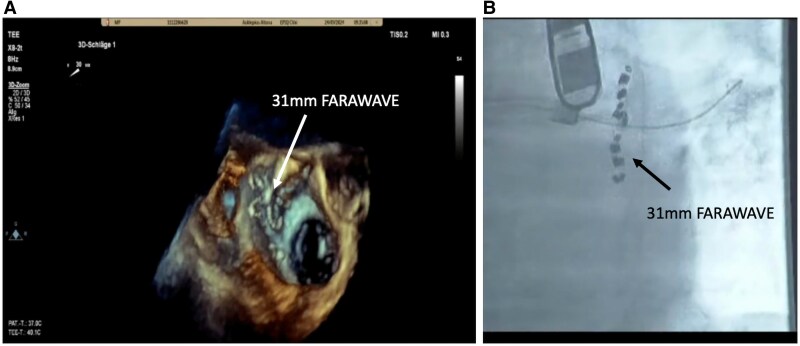
Case summary: In an 82-year-old male patient with symptomatic persistent AF, CHA2DS2-VA Score of 4 and HASBLED Score of 3 due to previous gastrointestinal bleeding were scheduled for a concomitant PVI + LAAC procedure. For minimum risk, a streamlined approach utilizing a single femoral vein puncture in combination with a suture-based closure system (Perclose Prostyle, Abbott) was performed. The transoesophageal echocardiography (TOE) LAA landing zone measurements were achieved directly prior ablation. Pulmonary vein isolation was performed with pentaspline PFA catheter (FARAPULSE). Although a swelling of the left atrial ridge was observed, a 24 mm WATCHMAN FLX device was successfully implanted. The patient was mobilized after 2 h and discharged on the next day. After 2 months on OAC, TOE found no gaps or leakage of the LAAC device and OAC was switched to acetylsalicylic acid monotherapy.
Discussion: A streamlined concomitant PFA-based PVI and LAAC procedure utilizing FARAPULSE and WATCHMAN FLX devices seems to be feasible and safe. Swelling of the ridge after PVI was observed; however, the sizing measurements have been performed prior PVI, and the LAAC procedure was successful with no evidence for gaps or leakage. A concomitant approach might be a suitable option for selected patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


