{"title":"Revised Ocular Trauma Score (rOTS): to develop and internally validate a predictive model for visual outcomes after open globe injury.","authors":"Parinee Kemchoknatee, Jayanton Patumanond, Somporn Chantra, Pennung Thongtong, Nattaporn Vongsa, Rinrada Kreesang, Dolchanok Dolman, Thansit Srisombut","doi":"10.1136/bmjophth-2025-002265","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We aimed to develop and validate a prognostic scoring model for predicting poor visual outcomes in patients with open globe injury (OGI).</p><p><strong>Design: </strong>A retrospective cohort study of patients with OGI from two teaching hospitals in Thailand.</p><p><strong>Methods: </strong>311 patients diagnosed with OGI between 2016 and 2023 were used to develop a multivariable logistic regression model predicting final visual acuity aimed at 6 months post-OGI. Visual outcomes were categorised into two groups using 20/200 as the cut-off for legal blindness. The model's performance was evaluated using receiver operating characteristic curve analysis. Internal validation was conducted with bootstrapping for 500 replications.</p><p><strong>Results: </strong>133 patients (42.77%) had visual acuity worse than 20/200 at the 6-month follow-up. The median follow-up time was 4.14 months, with an IQR of 3.00-11.74 months. Initial visual acuity (VA), relative afferent pupillary defect, rupture and eyelid injury were among the strongest predictors of visual outcome. Discrimination and calibration of the scoring model were satisfactory, with a C-statistic of 0.8671, a slope of 1 and a calibration-in-the-large of 0. Risk groups were created, categorised as mild, moderate and severe, with a C-statistic of 0.8094. The ORs for poor final VA (≤20/200) at 6 months were 1.51 (95% CI, 0.93 to 2.48) and 45.06 (95% CI, 11.20 to 387.94) in the moderate and severe risk groups, respectively.</p><p><strong>Conclusions: </strong>Our prognostic model (revised Ocular Trauma Score) can be seamlessly used in emergency settings to predict visual outcomes in patients presenting with OGI. Presenting visual acuity (VA) is the strongest predictor. Interpretation should be made with caution due to several limitations, including the predominance of severe cases inherent to a referral-based setting, the relatively small sample size and the absence of paediatric patients. External validation of our model is needed.</p>","PeriodicalId":9286,"journal":{"name":"BMJ Open Ophthalmology","volume":"10 1","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-08-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12359408/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjophth-2025-002265","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: We aimed to develop and validate a prognostic scoring model for predicting poor visual outcomes in patients with open globe injury (OGI).
Design: A retrospective cohort study of patients with OGI from two teaching hospitals in Thailand.
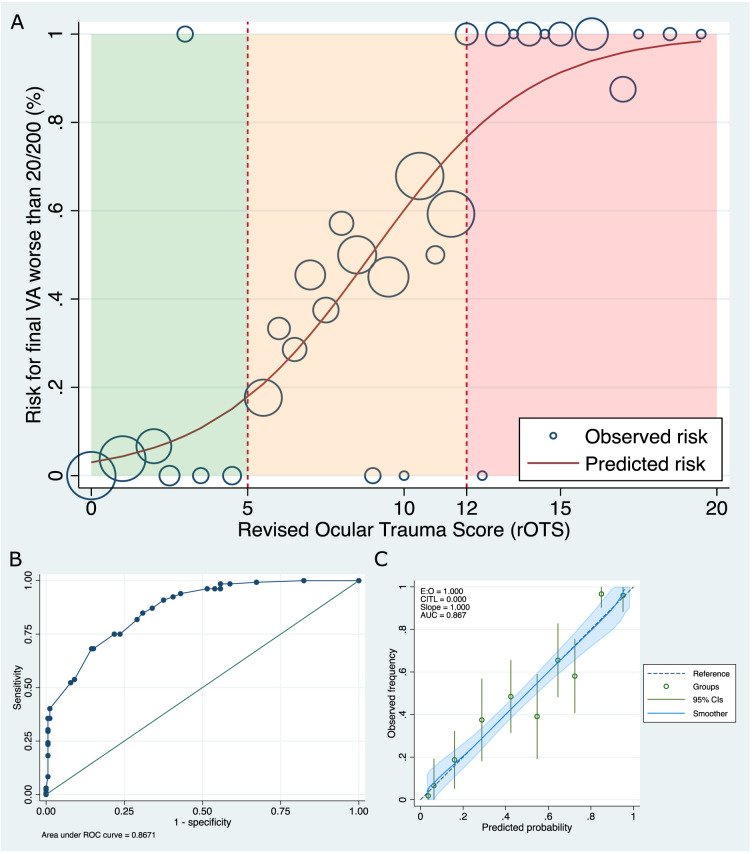
Methods: 311 patients diagnosed with OGI between 2016 and 2023 were used to develop a multivariable logistic regression model predicting final visual acuity aimed at 6 months post-OGI. Visual outcomes were categorised into two groups using 20/200 as the cut-off for legal blindness. The model's performance was evaluated using receiver operating characteristic curve analysis. Internal validation was conducted with bootstrapping for 500 replications.
Results: 133 patients (42.77%) had visual acuity worse than 20/200 at the 6-month follow-up. The median follow-up time was 4.14 months, with an IQR of 3.00-11.74 months. Initial visual acuity (VA), relative afferent pupillary defect, rupture and eyelid injury were among the strongest predictors of visual outcome. Discrimination and calibration of the scoring model were satisfactory, with a C-statistic of 0.8671, a slope of 1 and a calibration-in-the-large of 0. Risk groups were created, categorised as mild, moderate and severe, with a C-statistic of 0.8094. The ORs for poor final VA (≤20/200) at 6 months were 1.51 (95% CI, 0.93 to 2.48) and 45.06 (95% CI, 11.20 to 387.94) in the moderate and severe risk groups, respectively.
Conclusions: Our prognostic model (revised Ocular Trauma Score) can be seamlessly used in emergency settings to predict visual outcomes in patients presenting with OGI. Presenting visual acuity (VA) is the strongest predictor. Interpretation should be made with caution due to several limitations, including the predominance of severe cases inherent to a referral-based setting, the relatively small sample size and the absence of paediatric patients. External validation of our model is needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


