{"title":"Investigating inequality of childhood obesity in Bangladesh: a decomposition analysis.","authors":"Abdur Razzaque Sarker","doi":"10.1186/s40795-025-01018-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Due to rapid changes in global food systems, urbanisation, changes in lifestyle and dietary intake, many developing countries, including Bangladesh, are experiencing overweight-related issues among children and mothers. The aim of this study is to determine the prevalence of obesity among under-five children and to examine the factors that are potentially contributing to socio-economic inequalities of childhood obesity in Bangladesh.</p><p><strong>Methods: </strong>Data were extracted from the latest Bangladesh Demographic and Health Survey (BDHS) 2017-18 - a nationally representative cross-sectional survey which utilised a two-stage stratified sampling frame to cover the entire population of the country. Children under 5 years of age with weight-for-height-z-score (WHZ) > 3SD were defined as obese in this analysis. The concentration curve was plotted, and concentration indices (CIs) were calculated to observe inequality. A regression-based decomposition method was applied to assess the socioeconomic contributors to inequality in childhood obesity.</p><p><strong>Results: </strong>The overall prevalence of childhood obesity was 10.89% whereas the prevalence was higher among the urban children (14.27%) and the children aged 36 to 47 months of age (14.09%). Children of mothers with obesity (30.68%), small households (16.44%) and richest quintiles (15.19%) experienced the highest prevalence of obesity. The concentration curve lies below the line of equality and the value was 0.095 which implies that childhood obesity was highly concentrated among the upper (richer & richest) wealth quintiles. Wealth index of household (78.9%), childhood illness history (20.8%), overweight or obesity status of mothers (16.7%), administrative divisions (13.46%) and place of residence (10.4%) were the main contributors of the inequality of childhood obesity in Bangladesh.</p><p><strong>Conclusion: </strong>Disparities in childhood obesity remain a significant issue in Bangladesh and require urgent attention. Childhood obesity is more common among wealthier households and is linked to factors such as maternal obesity, childhood illness, and geographic location. Public health policies and interventions must address these risk factors to effectively combat childhood obesity across all segments of society.</p>","PeriodicalId":36422,"journal":{"name":"BMC Nutrition","volume":"11 1","pages":"164"},"PeriodicalIF":2.2000,"publicationDate":"2025-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12344960/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Nutrition","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40795-025-01018-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"NUTRITION & DIETETICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Due to rapid changes in global food systems, urbanisation, changes in lifestyle and dietary intake, many developing countries, including Bangladesh, are experiencing overweight-related issues among children and mothers. The aim of this study is to determine the prevalence of obesity among under-five children and to examine the factors that are potentially contributing to socio-economic inequalities of childhood obesity in Bangladesh.
Methods: Data were extracted from the latest Bangladesh Demographic and Health Survey (BDHS) 2017-18 - a nationally representative cross-sectional survey which utilised a two-stage stratified sampling frame to cover the entire population of the country. Children under 5 years of age with weight-for-height-z-score (WHZ) > 3SD were defined as obese in this analysis. The concentration curve was plotted, and concentration indices (CIs) were calculated to observe inequality. A regression-based decomposition method was applied to assess the socioeconomic contributors to inequality in childhood obesity.
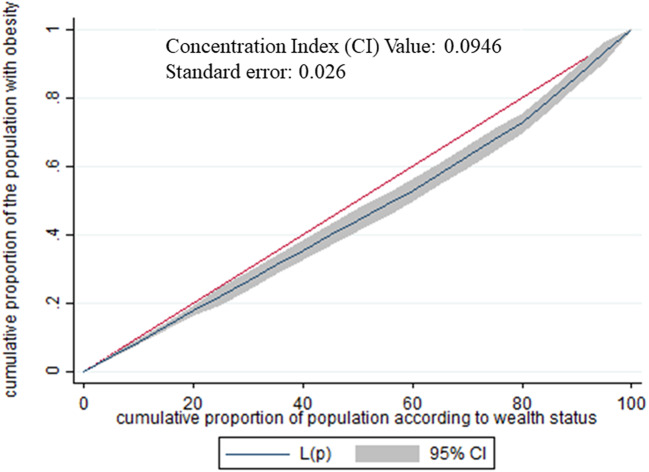
Results: The overall prevalence of childhood obesity was 10.89% whereas the prevalence was higher among the urban children (14.27%) and the children aged 36 to 47 months of age (14.09%). Children of mothers with obesity (30.68%), small households (16.44%) and richest quintiles (15.19%) experienced the highest prevalence of obesity. The concentration curve lies below the line of equality and the value was 0.095 which implies that childhood obesity was highly concentrated among the upper (richer & richest) wealth quintiles. Wealth index of household (78.9%), childhood illness history (20.8%), overweight or obesity status of mothers (16.7%), administrative divisions (13.46%) and place of residence (10.4%) were the main contributors of the inequality of childhood obesity in Bangladesh.
Conclusion: Disparities in childhood obesity remain a significant issue in Bangladesh and require urgent attention. Childhood obesity is more common among wealthier households and is linked to factors such as maternal obesity, childhood illness, and geographic location. Public health policies and interventions must address these risk factors to effectively combat childhood obesity across all segments of society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


